
Presentation
Headache and ophthalmoplegia. Increased prolactin levels.
Patient Data
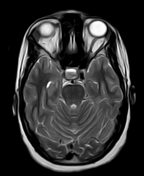

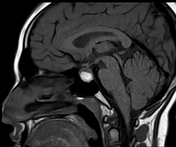
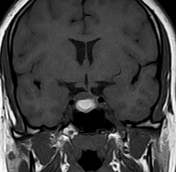
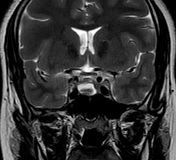
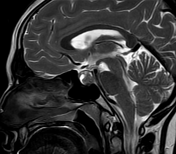
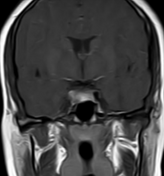
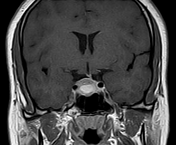
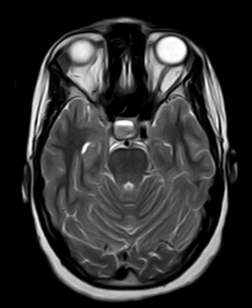
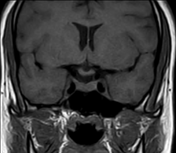
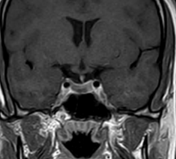
A sellar space occupying lesion mainly on the right side. It elicits cystic signal on T2 with internal haemorrhagic signal eliciting high signal on T1 and low signal on T2 WI. It shows marginal post-contrast enhancement. It shows upper contour bulge into the suprasellar region and causes mild sagging of the sellar floor and deviation of the pituitary stalk to the left side. No cavernous sinus invasion.
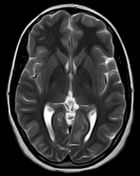
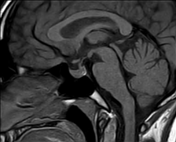
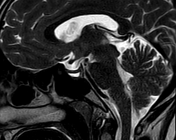
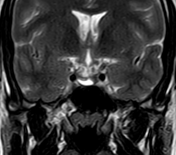
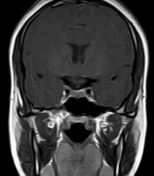
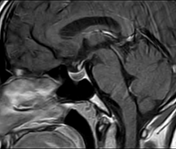
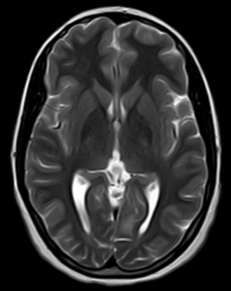
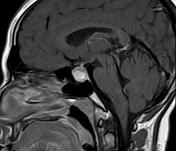
Follow-up MRI 6 months after medical treatment showed marked regression in size of the pituitary cystic lesion with resolution of the internal haemorrhagic signal. Currently, small intra-pituitary cystic lesion elicits low signal on T1 WI and high signal on T2 and appears less enhancing on the post-contrast series.
Case Discussion
Pituitary apoplexy is an acute clinical syndrome caused by either haemorrhage or infarction of the pituitary gland. Although variable, it typically comprises of headache, visual deficits, ophthalmoplegia, and altered mental status. An existing pituitary macroadenoma is usually present (60 - 90%) but it can occur with healthy glands in few isolated cases.
Pituitary apoplexy may also occur during pregnancy or post-partum period (Sheehan syndrome).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.