
Presentation
Status post right inguinal hernia repair with a mesh six years ago. Now has severe, sharp pain in the right groin radiating to the anteromedial thigh and erectile dysfunction. Hernia repair remains intact without evidence of recurrent hernia. EMG showed evidence of right-sided femoral neuropathy.
Patient Data
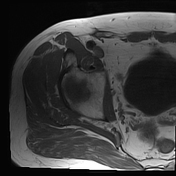

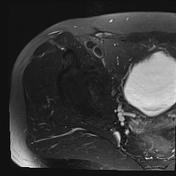
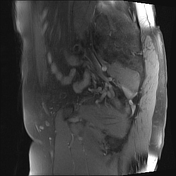

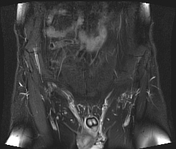
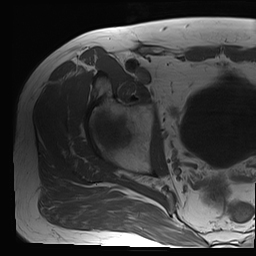
MRI of the pelvis shows scarring in the right inguinal region at the level of the inguinal ligament with mild thickening and hyperintensity of the ilioinguinal nerve as well as the genital branch of the genitofemoral nerve. This is best seen in the axial and coronal images (scarring, nerve hyperintensity). No compressive mass or fluid collection is seen.
Case Discussion
The genitofemoral nerve arises from the L1 and L2 spinal nerves and descends in the retroperitoneum into the inguinal canal. It bifurcates posterior to the ureter and forms the genital and femoral branches 1,2. The genital branch provides sensory innervation of the groin, genitalia, and pubic area, whereas the femoral branch innervates the skin of the anterior upper thigh 2.
Post-herniorrhaphy neuralgia presents as chronic neuropathic pain from the lower abdomen to the medial thigh due to iatrogenic nerve injury during herniorrhaphy. In males, it will present as scrotal pain, and in females, it will present as pain radiating to the labia majora and mons pubis 1. In our patient, inguinal hernia repair with mesh may have resulted in nerve injury during surgery and/or compression by scar tissue as shown on MRI, thus resulting in chronic pain. An additional etiology of our patient’s chronic pain to consider is the re-innervation of severed nerve remnants into the mesh used in surgery 3.
Our patient was started on gabapentin and biofeedback therapy. He was scheduled for image-guided right psoas compartment / genitofemoral nerve block although this was deferred as his symptoms improved with medications. If the chronic pain of post-herniorrhaphy neuralgia is refractory to medical treatment, laparoscopic triple neurectomy may be considered 4.
Case courtesy of Dr. Emad Allam - Assistant Professor of Radiology, Loyola University Medical Center


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.