
Presentation
Back pain radiating down to the right leg and fevers
Patient Data
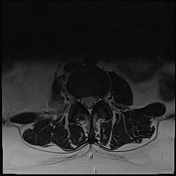

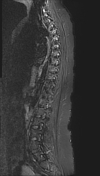
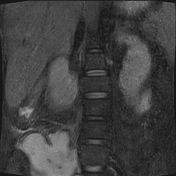
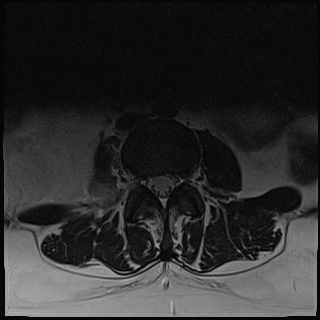
On axial T2 and coronal STIR, there is a partially imaged right-sided hyperintense retrofascial mass, encompassing and abutting the psoas major muscle. The mass appears to extend further inferiorly into the iliopsoas compartment and involves the quadratus lumborum muscle.
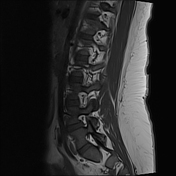
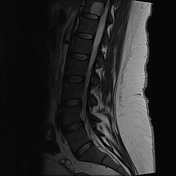
Well-defined hyperintense areas in the vertebral bodies of T11, L3 and S1 on sagittal T1 and T2, likely vertebral haemangiomas.
Normal morphology and enhancement of the spinal cord. Normal thoracolumbar alignment. No appreciable bone marrow oedema or infiltrates.
In the context of the noted history of fever and back pain, the most likely differential of this partially imaged mass would be a psoas abscess. Recommend CT abdominal pelvis with contrast for further characterisation.


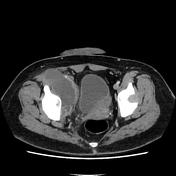
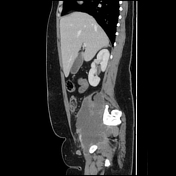


An extensive multiloculated right-sided hypodense collection extends antero-inferiorly from the psoas major and quadratus lumborum muscles into the inguinal region. Appreciable concomitant right-sided inguinal lymphadenopathy, likely reactive. Additional features of focal cellulitis around the right rectus femoris muscle. Given the clinical history and radiological findings, this represents a psoas abscess.
Case Discussion
The patient's presenting symptom was only severe back pain and right thigh/hip pain. The patient later developed a fever 48 hours after admission for what was initially suspected to be radicular back pain. MRI was originally performed to evaluate for potential osteomyelitis, which was later discovered as a psoas abscess.
The patient subsequently had an uncomplicated interventional radiology drainage of over 600 mL of pus with ongoing antibiotics. Isolates of meticillin-resistant Staphylococcus aureus (MRSA) were demonstrated on the intraoperative cultures. A PET scan was performed for evaluation of potential alternative sources of the abscess, however, it was concluded that the psoas abscess was the primary source.
Psoas abscess is a life-threatening diagnosis, requiring prompt treatment with antibiotics and consideration of drainage. Features of a psoas abscess on CT often include diffuse enlargement of the psoas muscle with an area of central low density.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.