
Presentation
Headache.
Patient Data
ASNR 2016: This case was submitted as part of the American Society of Neuroradiology (ASNR 2016) Case Of The Day competition, in collaboration with Radiopaedia.org.


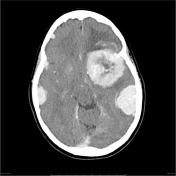
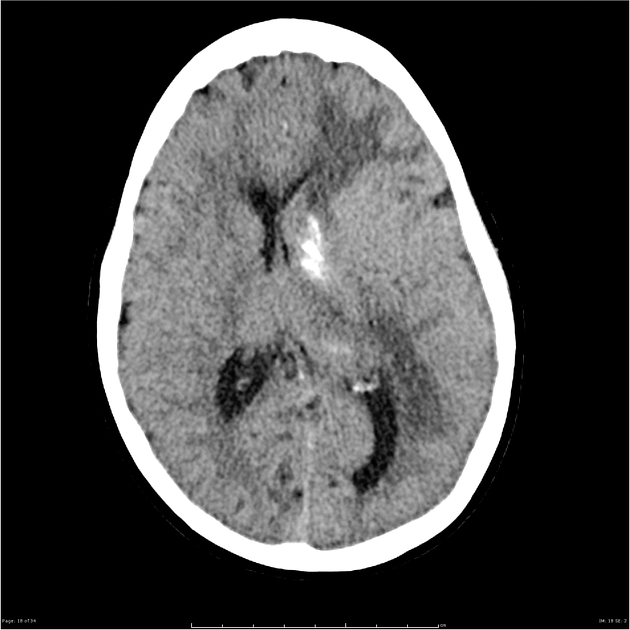
Numerous intra-cranial lesions, some presenting severe mass effect on the lateral ventricles. Prominent basal ganglia calcification. Post-contrast images demonstrated vivid enhancement, homogenous in smaller masses and heteregenous in larger masses.

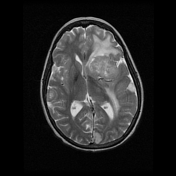
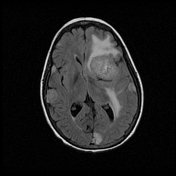
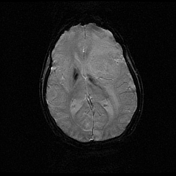
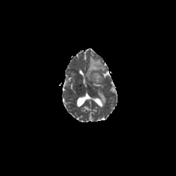
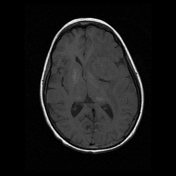
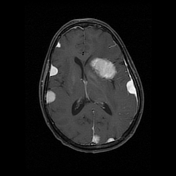
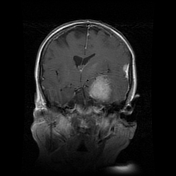

Numerous (approximately 20) intracranial, supratentorial, bilateral masses are noted. The largest is centred on the junction of the left anterior and middle cranial fossa, and demonstrates (to gray matter) iso-intense T1 signal, heterogenous iso/high T2/FLAIR signal and vivid high post-contrast T1 FS signal with internal flow voids indicative of blood vessels.
Other lesions demonstrate similar characteristics (some small lesions lack internal flow voids). Masses appear to be extra-axial as they distort overlying cerebral gyri and sulcli and many demonstrate a dural tail. High T2/FLAIR signal noted within the white matter of the left cerebral hemisphere, consistent with vasogenic oedema.
The largest masses are on the left and along with vasogenic oedema produce left-to-right midline shift of approximately 4mm and result in significant partial effacement of the left lateral ventricle and mild left uncal herniation.
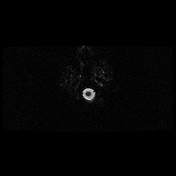
No susceptibility artefact to indicate haemorrhage. No diffusion restriction. Basal ganglia calcification is noted.
Conclusion:
Findings are consistent with multiple meningiomas. It is unlikely that these dural masses represent metastases, particularly in view of the spoke-wheel blood supply demonstrated in the largest lesion.
The patient proceeded to craniotomy and resection of the largest lesions.
Histopathology
MACROSCOPIC DESCRIPTION: 1. "Brain tumour": Two pieces of firm tissue, each 4mm. All in for frozen section. FS DIAGNOSIS: Meningioma - some nuclear atypia (AET). A1. 2. "Brain tumour": An ovoid piece of soft pink fawn tissue 27x14x10mm with attached grey membranous tissue 11x7x1mm at one edge of the specimen. TS x9. A2. (SWB) 3. "Posterior temporal tumour": A portion of brain tissue 36x26x17mm. A6. 4. "Left sphenoid tumour": Multiple fragments of soft and rubbery tan tissue measuring in aggregate 35x35x15mm. A5. (MAS)
MICROSCOPIC DESCRIPTION: 1-4. The sections show moderately cellular tumours with infiltration into the attached dura. They form fascicles and whorls. No sheeting arrangement is seen. The tumour cells have moderately enlarged nuclei and focal conspicuous nucleoli. There is 1 mitosis per 10 high power fields. The blood vessels contain foreign body material, consistent with preoperative embolisation. There is no necrosis. No brain parenchyma is seen. The tumour cells are EMA and PR positive. The Ki-67 index is about 3%. The features are those of meningiomata. There are insufficient features for atypical or malignant change.
DIAGNOSIS: 1-4. Brain tumours: Meningiomata (WHO Grade I).
Case Discussion
This patient had a history of ALL as an infant treated with chemotherapy and whole brain radiotherapy.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.