
Presentation
Dizziness.
Patient Data
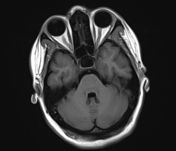


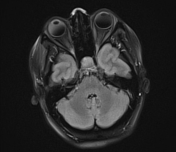
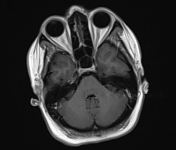

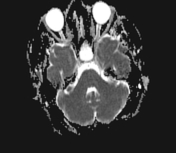
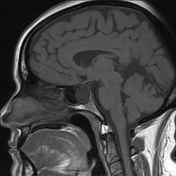
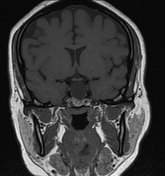

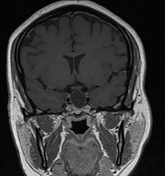
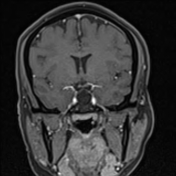

An expanding sellar cystic lesion is seen averaging 2 x 1.6 cm. It is homogeneous hypointense on T1, hyperintense on T2 and of high signal on FLAIR. No enhancing soft tissue component. it is completely marginated by stretches and compressed thin rim of pituitary tissue reflecting intrapituitary lesion. It is abutting the ICAs bilaterally in cavernous sinuses.
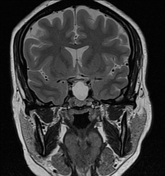
Hairline plane of cleavage from the optic chiasms, with central pituitary stalk. The sellar cystic lesion is extending to the suprasellar cistern. Scalloping of sella floor is also noted.
Case Discussion
The patient did CT study before this examination which noted an empty sella turcica, unlike the MRI appearance of the intrasellar cyst.
In this case, It follows CSF signal in all pulse sequences except FLAIR which shows hyperintensity. The surrounding enhancing rim is the compressed pituitary gland, which confirms intrapituitary location. It is uncommonly to see Rathke cleft cyst reaching the suprasellar cistern.
Rathke cleft cyst is seen as an intrasellar well-defined non-enhancing midline cyst, arising between the anterior and intermediate lobes of the pituitary gland. It becomes symptomatic if compressed pituitary gland affecting its functions, some cases present with hormonal disturbance (e.g. hyperprolactinemia).
Differential diagnosis includes intrasellar arachnoid cyst and cystic pituitary adenoma. The central infundibulum excludes arachnoid cyst and absence of any mural component excludes cystic pituitary adenoma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.