
Presentation
Left lateral chest wall lump, pulsatile and expansile on clinical exam.
Patient Data
CT chest with contrast


Contrast-enhanced exam. No previous cross-sectional imaging for comparison.
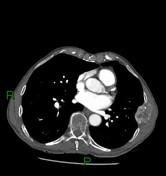
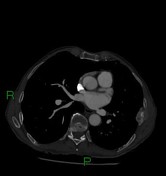
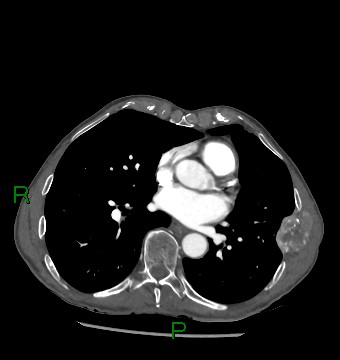
Heterogeneously but relatively avidly enhancing soft tissue mass lesion centered on the left lateral seventh rib, measuring 44 x 33 mm in greatest transaxial dimensions, with associated underlying rib destruction.
A few scattered foci of cystic change in the lungs, of doubtful significance. Bibasal atelectasis. Lungs are otherwise clear with no concerning pulmonary nodules.
Previous total gastrectomy noted. Irregular focus of hypoattenuation at medial aspect of liver, may represent a perfusional abnormality. Simple left renal cyst in the partially imaged left kidney. Normal spleen and pancreas. Normal left adrenal. No other destructive bony abnormality demonstrated. No size significant lymph node enlargement in the scanned volume.
Aneurysmal celiac trunk, measuring 15 mm in diameter, with thin peripheral calcification.
Opinion:
Centered on the left lateral seventh rib is an enhancing destructive mass lesion, appearance is highly concerning for malignancy, most likely a metastasis.
Contrast-enhanced CT abdomen and pelvis is suggested to further assess.
Incidental aneurysmal celiac trunk.
I note prior history of total gastrectomy and previous bowel resection with stoma reversal (presumably around left splenic flexure given presence of hyperdense suture material).
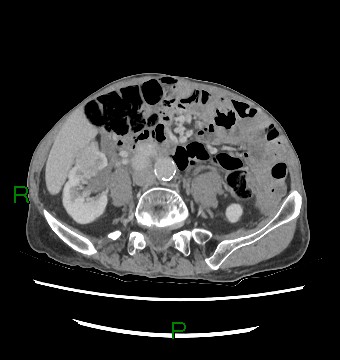
Within the inferior pole of the right kidney, there is a lobulated soft-tissue density mass measuring approximately 45mm AP x 52 mm TR x 66mm CC. Foci of hypoattenuation within this mass could be in keeping with central necrosis. There are several surrounding enlarged lymph nodes anterior to IVC. In particular there is some central hypoattenuation in a 21mm node, in keeping with a necrotic-looking lymph node.
Hepatic cyst. Otherwise normal liver, adrenals, spleen and pancreas. An enlarged prostate indents the base of the bladder.
Suboptimal assessment of bowel loops due to paucity of abdominal fat. Prominent loop of dilated transverse colon which measures up to a maximum of 7.5cm but no evidence of obstructing lesion downstream. No free fluid or air within abdomen or pelvis.
Scattered centrilobular and paraseptal emphysema. Minor bibasal linear atelectasis. No destructive bony lesions.
Opinion:
Right inferior pole renal soft-tissue density mass, likely in keeping with renal malignancy. Associated surrounding enlarged lymph nodes.
Case Discussion
There is a limited differential for expansile vascular bony metastases, namely:
- renal cell carcinoma
- thyroid cancer
- hepatocellular carcinoma
- pheochromocytoma
- melanoma
- gastric carcinoma
For this specific case, the gastrectomy was performed due to adhesions secondary to previous colonic resection for colorectal cancer rather than gastric carcinoma.
The rib metastasis was subsequently biopsied, histopathology is in keeping with metastatic clear cell renal cell carcinoma, which is the most common type of renal cell carcinoma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.