
Presentation
Severe headache after minor head trauma. No vomiting or loss of consciousness.
Patient Data

There is a crescentic CSF density accumulation in the left subdural space extending to the large similar density extra-axial cystic structure seen in the left temporoparietal region/middle cranial fossa.
Mass effect is noted with a mild shift of midline.
Thinning of the adjacent calvarial bone indicating a slow longstanding process.
No intracranial hemorrhage is seen.
No depressed skull vault fracture is seen.
The visualized paranasal sinuses and mastoid air cells are clear.
Features are in keeping with ruptured left temporal arachnoid cyst with subsequent subdural hygroma causing mass effect and shift of midline ( type III according to Galassi classification).
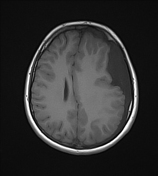


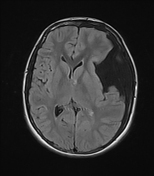
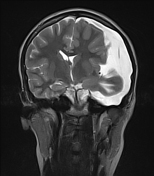
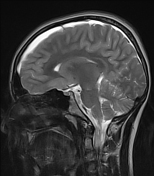

There is a large CSF intensity area seen occupying the left temporal fossa and replacing most of the left temporal lobe, suggestive of a large left temporal fossa arachnoid cyst, associated with diffuse subdural hygroma /subdural effusion surrounding the left cerebral convexity and appears to be continuous with the above-mentioned arachnoid cyst, there appears to be causing mass-effect upon the cerebral parenchyma with the shifting of the midline structures towards the right side ( about 8mm off the midline ) findings are consistent with ruptured arachnoid cyst with subsequent subdural hygroma.
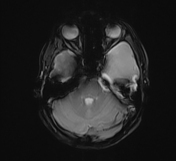
No obvious intracranial hemorrhage or acute infarcts. No evidence of hydrocephalus. Normal brainstem and cerebellum.
Case Discussion
In this case, the presence of an arachnoid cyst was discovered incidentally after imaging for persistent headache following head trauma. Imaging reveals a large arachnoid cyst (type III) with associated ipsilateral subdural hygroma likely due to traumatic rupture.
Arachnoid cyst is a common intracranial pathology, usually asymptomatic. It follows the CSF density and intensity on CT and MRI respectively with possible adjacent bone remodeling.
The most common location is the middle cranial fossa which is calcified into three types according to their size, Galassi classification. Rupture into the subarachnoid space is a rare complication.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.