
Presentation
Recent onset of thoracic back pain. Previously well.
Patient Data


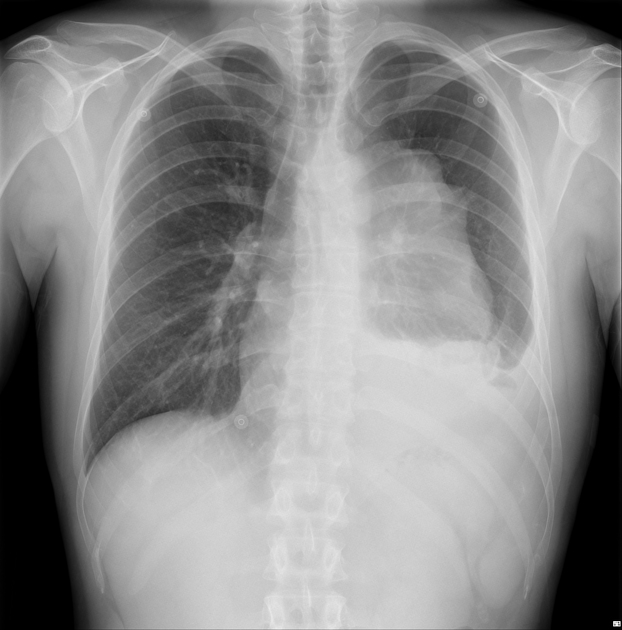
Large lobulated mass in the medial left mid-zone.
Left-sided pleural effusion with passive atelectasis.
Tracheal deviation to the right.




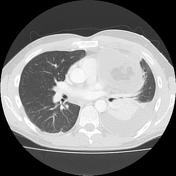
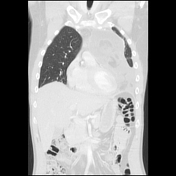
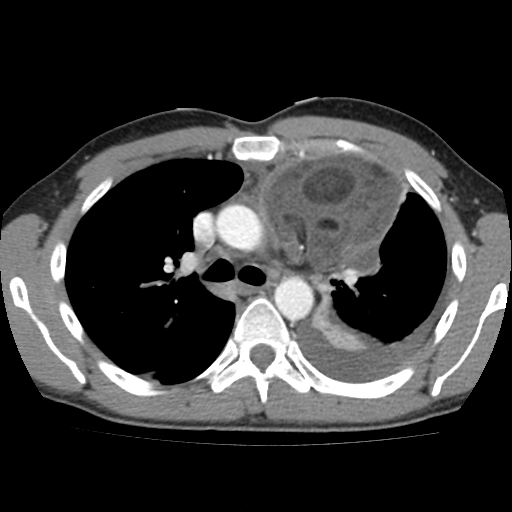
Heterogeneous fat and fluid attenuation in a left-sided anterior mediastinal mass measuring 15 cm in craniocaudal length and closely applied to the mediastinum and pericardium. It extends from the left subclavian vein superiorly to the pericardium, close to the diaphragm.
Multiple fatty and nodular components within the mass.
The mass is less well defined inferiorly compared to the well-defined capsule superiorly.
Possible site of rupture inferiorly marked by fatty tissue and track.
Moderate compression of the left main bronchus and mediastinal shift to the right.
Moderately large left pleural effusion.
The right lung is clear.
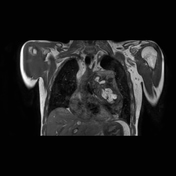
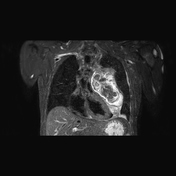
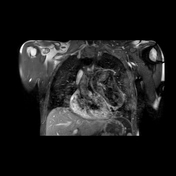
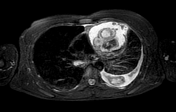
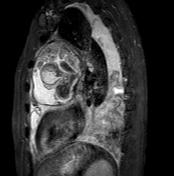
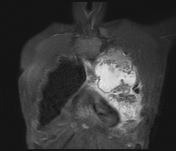
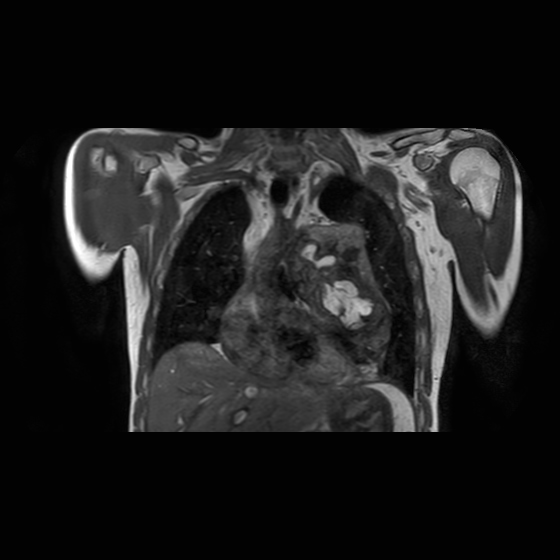
15 cm heterogeneous mass with fat components occupies the anterior left mediastinum. Its superior portion is well encapsulated. Mass effect with moderate narrowing of the left main bronchus. The mass extends inferiorly beyond the well-encapsulated portion, adjacent to the left heart border and extending into the mediastinal fat. This suggests rupture of the tumor beyond the capsule abutting the left pericardium and measures up to 8.1 cm craniocaudally. The mass abuts the anterior chest wall without invasion.
Moderately large left pleural effusion. No enhancing pleural nodules.
Right lung clear. Mild shift of the mediastinum to the right.
Pre-operative serum alphafetoprotein and beta HCG were in the low normal range.
SURGERY:
Incision: antero-lateral thoracotomy (left).
Findings: mass measuring 15 cm, adherent to pericardium, part of lung tissue, left subclavian vein.
Resection of mass and plication of diaphragm.
Resection of part of lung tissue.
Resection of part of pericardium and repair with Gortex patch.
Drains: left apical and basal.


Macroscopic description: Mass measuring 230 x 90 x 85mm. The cut surfaces reveal a multicystic cavity, containing firm pale material with adipose tissue and hair, and loose pale friable material.
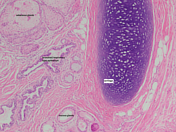
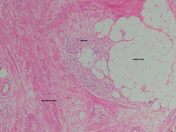
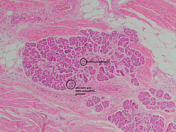
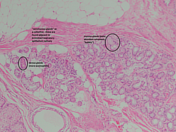
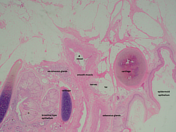
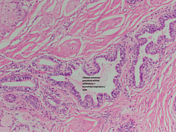
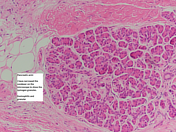
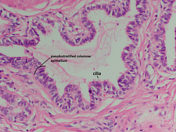
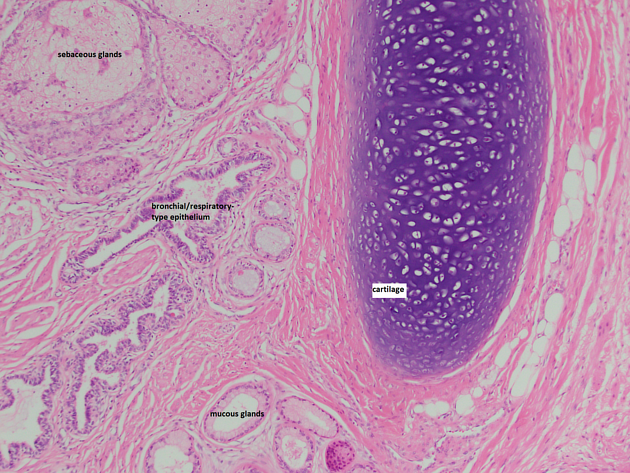
Microscopic description: The mass lesion is a benign cystic teratoma. The tumor is largely composed of a cyst lined by mature squamous epithelium and numerous foamy macrophages, foreign body type multinucleated giant cells and granulation tissue with keratin material in the cystic space. The tumor also contains a solid area of mature skin, mucinous glands, pancreatic glands, and mature cartilage. No immature tissue or malignancy is found.
(Zymogen granules are annotated. These are storage granules found in exocrine pancreatic tissue.)
DIAGNOSTIC SUMMARY:
1. Fourth rib margin left: No tumor.
2. Anterior pericardial dissection margin: No tumor
3. Mediastinal mass: Benign cystic teratoma. No evidence of malignancy.
4. Lymph node station 6: No evidence of malignancy.
Case Discussion
About one-quarter of adult teratomas are located in the anterior mediastinum and may be derived from primordial thymic cells. They are usually benign, slow-growing tumors commonly containing well-differentiated exocrine pancreatic tissue. Autodigestion may account for the propensity to rupture, and amylase can be found in aspirates from the tumor and pleural fluid 1-3. In contrast, malignant teratomas contain poorly differentiated tissue and are less likely to rupture. Elevated AFP and/or β-hCG are markers of malignancy, both of which were negative in this case.
In this case, the mass was predominantly cystic and contained mature skin, mucinous glands, pancreatic glands, mature cartilage, adipose tissue and hair. The rupture caused inflammation, adhesions, and pleural effusion, necessitating resection, including the adherent pericardium and lung.
Labeled pathology courtesy of Dr Alexander va Laar Veth.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.