
Presentation
Lytic sacral mass of unknown origin (X-rays not available).
Patient Data







Lytic sacral lesion with a large lobular soft tissue component hypodense to muscle, measuring 7.9 x 5.6 x 5.0 cm, involving S2-S4 and obliterating the foramina.
Old left upper and lower pubic rami nonunion fractures.
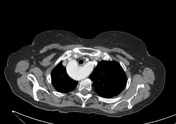
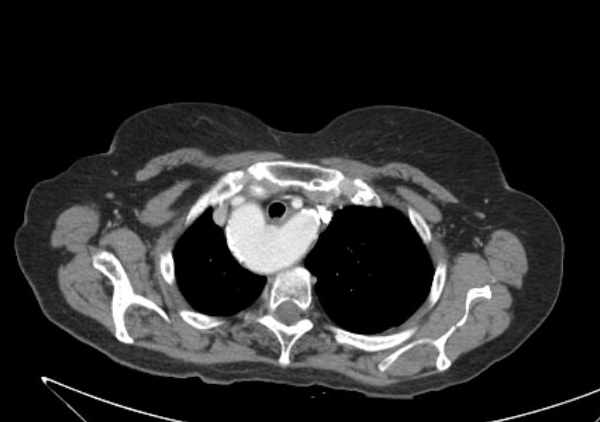
Right aortic arch.
Tiny subpleural nodule in the LUL apicoposterior segment.
Diverticulosis of the descending and sigmoid colon.
The urinary bladder is overly distended - consider catheterisation.




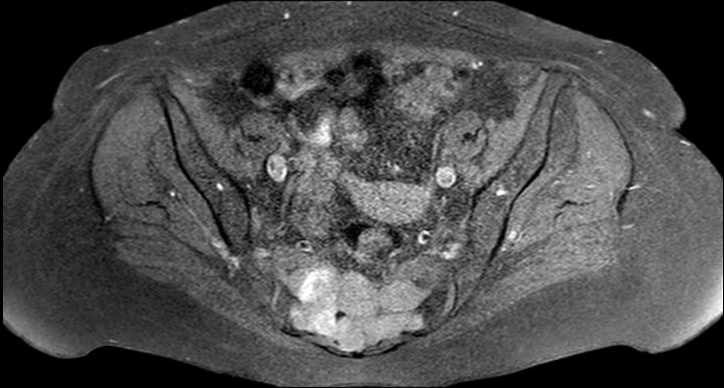
The soft tissue component of the sacral mass appears hyperintense on all sequences.
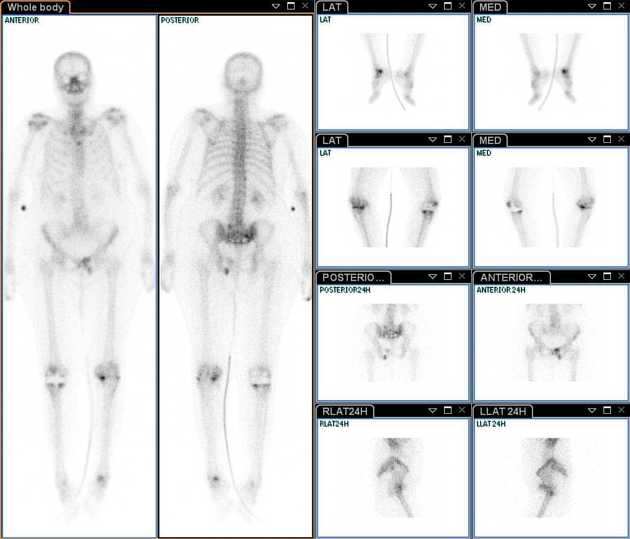
Photopenic area in the sacrum with increased radiotracer uptake in its periphery and the lower part of the right sacroiliac joint, compatible with a neoplastic lesion.
Increased uptake in left superior and inferior pubic rami, in keeping with fractures.
Increased uptake in the lumbar spine, particularly L5 on left, signifying degenerative changes.
Status post right knee replacement. Increased uptake around the implant, particularly in the patella and the medial tibial component - can signify either loosening or infection.
Increased uptake in the left knee in the medial articular area - can signify arthritic changes with suspected damage to the medial meniscus.
Increased uptake in the area of the left talus - the character of uptake suggests trauma.
Case Discussion
Highest on the differential list are:
- chordoma - midline tumour
- solitary bone plasmacytoma, multilocular type
- giant cell tumour - not likely, given the patient's age
- metastasis - unlikely, as no other tumour was detected on CT or SPECT
Unfortunately, the pathology report is unavailable.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.