
Presentation
The patient presented with occasional pain on the right side of the neck, especially during exercise, for 4 months.
Patient Data
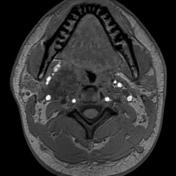


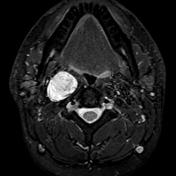
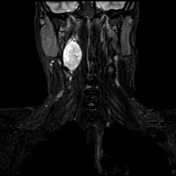
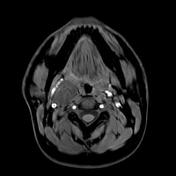


A well-defined ovoid encapsulated lesion appearing heterogeneously T2, STIR hyperintense and T1 hypointense in the right post-styloid parapharyngeal space, medial to the carotid space. The lesion measures 4 x 2.4 x 2.6 cm (CC x AP x ML), over C1-C3 levels. No evidence of flow voids within the lesion. The lesion is longitudinally orientated without neural foraminal extension. There is no arterial phase enhancement. In the delayed phase, the lesion shows homogeneous enhancement.
The lesion displaces the internal carotid artery and internal jugular vein laterally (in the same direction) without separating nor encasing the vessels.
The lesion is anterior to the ipsilateral longus capitis and longus coli muscles.
There is no frank evidence of local invasion.
Case Discussion
Schwannomas of the head and neck are slow-growing tumours, usually presenting as asymptomatic masses. Most of the extracranial schwannomas arise in the parapharyngeal space and are usually of vagal origin. Meanwhile, Schwannoma of the cervical sympathetic chain (SCSC) is a rare entity.
The vagus nerve courses between the IJV and ICA along the entirety of the carotid sheath; hence schwannomas of vagal origin tend to separate these vessels. The cervical sympathetic chain is found posteromedial to ICA and IJV; therefore schwannomas of the cervical sympathetic chain will not separate these vessels. SCSC can rarely splay the CCA bifurcation without encasing ICA and ECA.
Teaching point, in this case, is that schwannoma of the cervical sympathetic chain has a propensity to displace ICA and IJV in the same direction, while vagal schwannoma displaces them in opposite direction.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.