
Presentation
Right-sided myoclonic jerking.
Patient Data
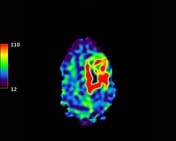

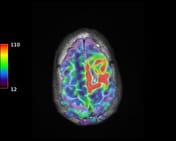
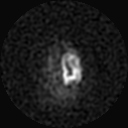
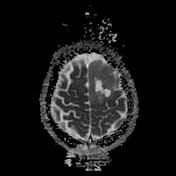
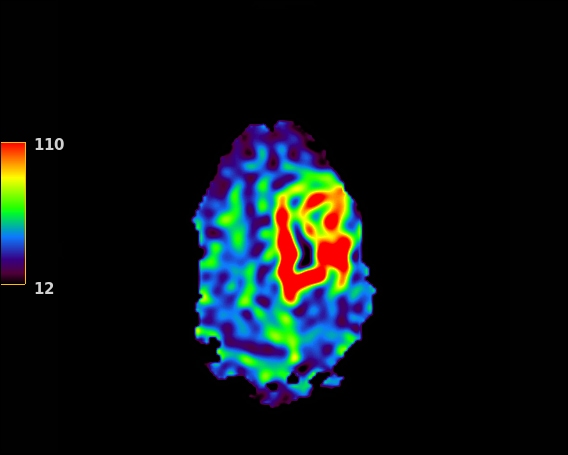
Arterial spin labeling (ASL) shows markedly increased cerebral blood flow (CBF) within and surrounding a lesion in the left frontal lobe along with relative hypoperfusion in the right cerebellar hemisphere. In a patient with clinical seizure activity, these findings are suggestive of seizure with crossed cerebellar diaschisis. While there is some relative hyperperfusion in both thalami, this can be seen in normality as well as in seizure.
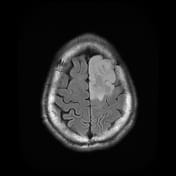
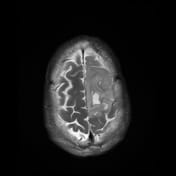
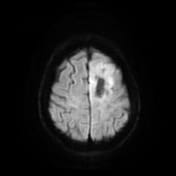
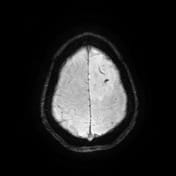
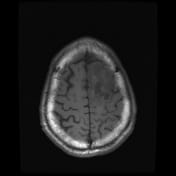
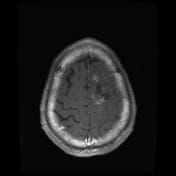
The seizure focus centers around a previously treated astrocytoma with radiation necrosis and hypoperfusion (on previous external imaging). The surrounding gyral thickening, extensive T2 FLAIR signal hyperintensity, post-contrast enhancement and foci of susceptibility artefact were all stable at the time of imaging.
Case Discussion
Electroencephalogram (EEG) subsequently showed an asymmetric slowing in the left paracentral region with periodic epileptiform discharges (PLEDs) which were broad-based, phase-reversing and variable in frequency consistent with electrographic partial seizures.
This case with clinical seizure activity demonstrates arterial spin labeling (ASL) and EEG findings supportive of the ictal phase of seizure 1.
Crossed cerebellar diaschisis is thought to arise in the acute setting as a result of excessive excitatory input from the seizing cortex to the contralateral cerebellar hemisphere via corticopontocerebellar pathways 2.
In the months following this acute presentation, interictal imaging unfortunately highlighted new areas of hyperperfused high grade tumor recurrence. In this regard, the ASL findings on the current study likely represent a combination of both seizure and new recurrent high grade tumor which subsequently came to light at follow up.
Case courtesy of Professor David Ryan (Cork University Hospital).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.