
Presentation
Lump on head.
Patient Data









Destructive soft tissue mass involves the frontal bone on the left.










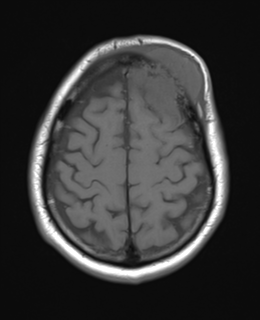
Pre and post IV contrast multiplanar imaging of the brain has been performed. There is a large mass centred within the anterior left frontal bone. This is a destructive mass with a small amount of tumour extending into the extra-axial space with associated local mass-effect. There is lifting of the underlying dura which demonstrates smooth contrast enhancement beyond this. There is a much larger subcutaneous component of the mass lesion. No other bony lesions identified. No intra or extraaxial haemorrhage identified. No signal abnormality evident. No restricted diffusion.
Conclusion:
Mass most likely represents a metastasis. Meningioma and haemangiopericytoma are differential diagnoses, but less likely.
Case Discussion
The patient had a history of prior lung malignancy, and went on to have skull surgery.
Histology
MICROSCOPIC DESCRIPTION: Paraffin sections show a densely hypercellular epithelial tumour involving brain parenchyma. Tumour cells have large round and oval vesicular nuclei, many with conspicuous nucleoli and a variable amount of pale cytoplasm. These are arranged in solid sheets in a vascular stroma. Frequent mitotic figures are identified and there are multiple foci of tumour necrosis. Immunohistochemistry shows strong cytoplasmic staining in tumour cells for pancytokeratin AE1/AE3, cytokeratins CAM5.2 and CK7 and for carcinoembryonic antigen (CEA) and BerEp4. There is also strong nuclear staining for p40 and p63. No staining for TTF-1, Napsin A or tyrosinase is seen in tumour cells.
FINAL DIAGNOSIS: Metastatic undifferentiated non-small cell carcinoma with features favouring poorly differentiated squamous cell carcinoma and most consistent with an origin from lung.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.