
Presentation
Recent subclavian TAVI, new tense abdomen and serum lactate 3.
Patient Data





Non-contrast and arterial phase CT chest, abdomen, pelvis, followed by portal venous phase CT abdomen and pelvis.
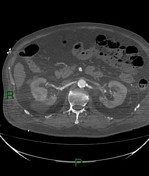
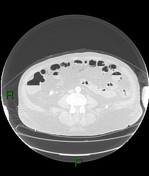
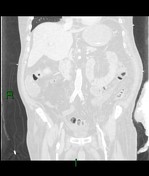
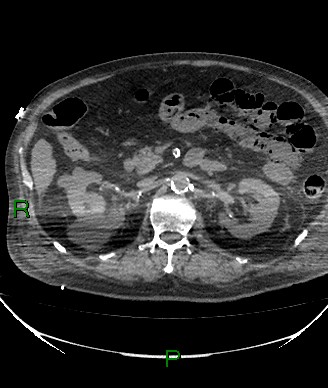
Extensive small bowel intramural gas and gas within the mesenteric veins. No main portal venous gas or gas within the liver.
Small volume of pelvic free fluid.
The superior mesentery artery opacifies normally (non-occlusive proximal thrombus noted).
Normal liver, adrenals, pancreas and spleen. Possible small gallstones in gallbladder. Multiple bilateral simple renal cysts.
Severe calcified abdominal aortic disease.
Moderate left pleural effusion. Small right pleural effusion.
Left lower lobe is most entirely collapsed. 14 mm nodule in left upper lobe. Right lower lobe atelectasis.
Prosthetic aortic valve in situ. Possible trace pericardial effusion.
Left subclavian artery stent.
Satisfactory positions of the right internal jugular central venous catheter, nasogastric tube and endotracheal tube.
No concerning bony abnormality.
Opinion:
Extensive small bowel infarction with extensive mesenteric venous gas. Superior mesenteric artery is opacifying normally. Likely aetiology is multiple trash emboli.
Case Discussion
This case highlights the importance of reviewing CT abdomen and pelvis examinations in lung windows, and appreciating the gas is conforming to curvilinear configurations which are contiguous with the mesenteric veins, as well as the non-dependent gas confined to the small bowel wall.
Within the context of recent aortic valve intervention which is likely to have had underlying calcified disease, and the absence of occlusive superior mesenteric artery thrombus, trash emboli would be the most likely aetiology.
Unfortunately the patient did not survive the acute insult.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.