
Presentation
Left-sided hemiplegia. No history of trauma or prior surgery.
Patient Data
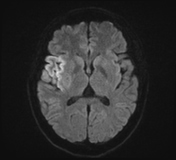

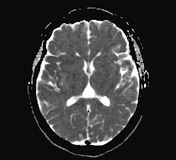
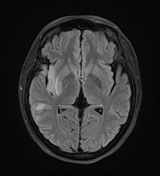
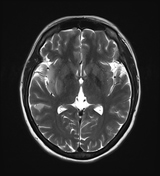
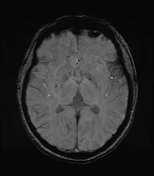
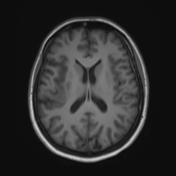
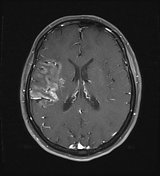
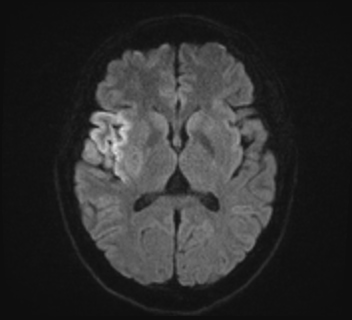
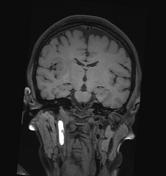
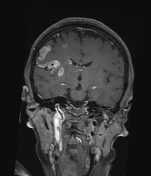
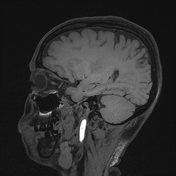
Subacute cerebral infarctions scattered within the frontal, temporal, parietal lobes, putamen, corona radiata, and right insular lobe, with diffusion restriction and post-contrast enhancement in a gyriform pattern.
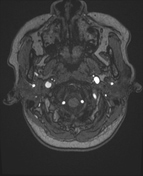
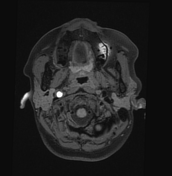
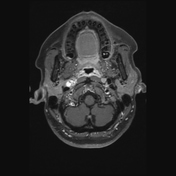
Hyperintense signal in the right extracranial internal carotid artery on T1W, T2W, and FLAIR sequences, with diffusion restriction and signal drop out and blooming on SWI, suggestive of thrombus.
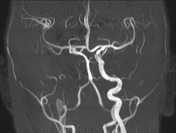
On MRA, absent flow signal in the right internal carotid artery from the C2 to C7 segments, with intraluminal hyperintensity in the C1 segment (extracranial portion), suggestive of thrombosis causing severe luminal narrowing. Flow within the right anterior cerebral artery and middle cerebral artery are still preserved, receiving supply from the anterior communicating artery and right posterior communicating artery.

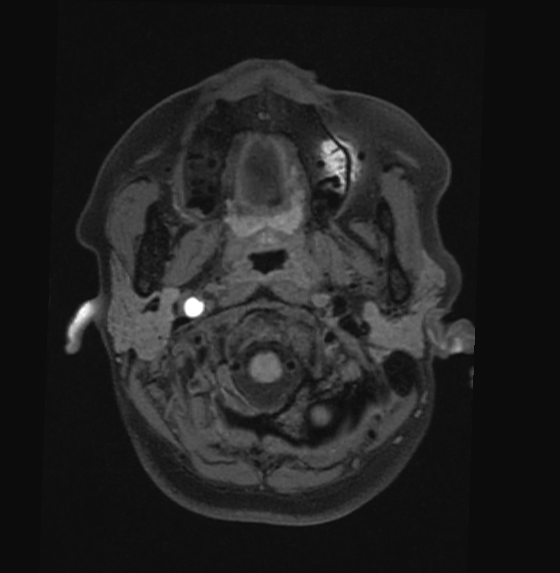
On VM-MRI, the following findings are noted:
right internal carotid artery dissection at the extracranial C1 segment, with a visible floating intimal flap and intramural hematoma measuring approximately 7 x 7 x 32 mm, causing severe luminal narrowing; reduced flow in intracranial segments from C2 to C7, accompanied by diffuse wall enhancement
asymmetric eccentric wall thickening (crescent sign) of the left vertebral artery in the extracranial segment, with high signal intensity on T1FS, no clear contrast enhancement, and mild luminal narrowing, suspected dissection
Case Discussion
The imaging findings are consistent with subacute cerebral infarction secondary to internal carotid artery (ICA) dissection.
Case co-author: Consultant specialist Tran Quyet Thang, Military Hospital 175, Vietnam.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.