
Presentation
Severe epigastric pain and hematemesis.
Patient Data




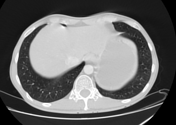

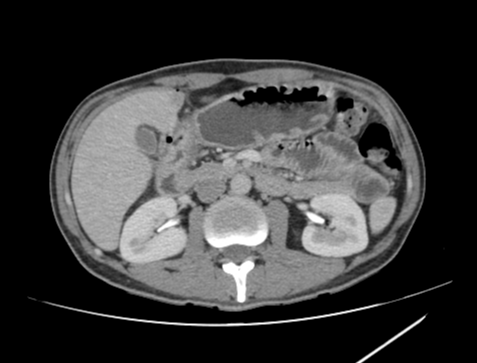
The gastric pyloric antrum and 1st duodenal segment show mural thickening with mucosal enhancement, submucosal edema, and air loculi passing through the wall likely through ulcer defect, associated with subtle pneumoperitoneum with extragastric air loculi and air loculi abutting the hepatic dome adjacent to the IVC and the anterior hepatic surface, evident on lung window. Right perigastric fat plane smudging extending to the pericholecystic planes, representing focal peritonitis.
Findings are suggestive of a perforated distal gastric pyloric antral ulcer with pneumoperitoneum and right focal peritonitis.
Case Discussion
The case shows subtle findings of gasric ulcer perforation including distal gastric pyrloic antral and 1st duodenal segment mural thickening with mucosal enhancement and submucosal edema as well as subtle pneumoperitoneum and mild focal peritonitis. It was misdiagnosed as a normal study by the attending radiology trainee.
In patients presented to ER with acute epigastric pain and/or hematemesis, you have to check the gastric antrum and first duodenal part carefully for abnormal mural thickening, enhancement and submucosal edema as well as wall defect (ulcer). Also, lung window is crucial for detection of subtle pneumoperitoneum. Finally, You must carefully look for abnormal fluid collections or peritoneal/omental fat plane smudging and stranding, which are indicators of focal peritonitis.
Following immediate surgical intervention, the diagnosis of distal gastric pylroic antral ulcer perforation was established.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.