
Presentation
Sudden onset right sided face (including lip and tongue), arm and leg tingling. Persistent and non- progressive. Nil other neurological symptoms such as headache, visual changes or weakness/numbness. No trauma or loss of consciousness. No preceding symptoms. Nil increased stressors, infective symptoms, fever or rashes. No night sweats or weight loss.
Patient Data
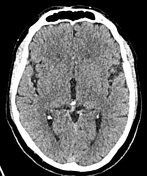



No acute intracranial hemorrhage identified. No intra- or extra-axial collection.
No focal mass identified within the limits of CT. The basal cisterns are clear. The sulcation pattern is normal for age. No hydrocephalus. The sellar and parasellar structures are unremarkable. No cerebellar tonsillar descent.
No destructive skull bone lesions identified. No fracture of the skull vault or skull base identified.
The aortic arch does not demonstrate significant stenosis with no dissection flap seen.
The common carotid arteries bilaterally are widely patent with no significant stenosis or dissection identified.
The internal carotid arteries demonstrate no significant stenosis or appreciable dissection.
The vertebral arteries demonstrate no significant stenosis or appreciable dissection.
The basilar artery is patent.
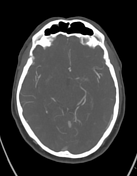
No occlusion of the proximal branches of the circle of Willis seen.
Specifically A1-A2, M1-M2 and P1-P2 are patent with no significant stenosis identified.
No intracranial aneurysm identified
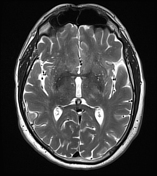
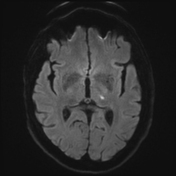
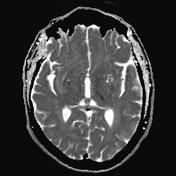
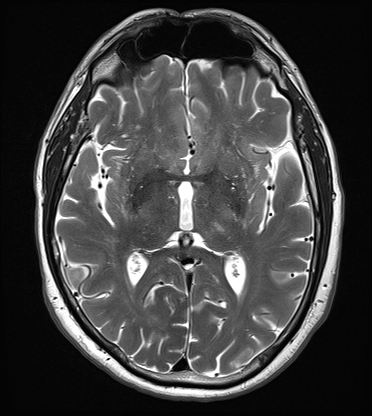
There is a left thalamic small area of diffusion restriction. It is likely to interrupt sensory tracts from the right hemi-body.
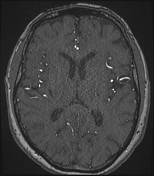
Time of flight MRA shows a large right vertebral artery, slender left. Left vertebral artery terminates as the PICA. This is still a normal variant. Basilar is flowing.
Both posterior cerebral arteries are flowing, both P1 segments are flowing. The area of infarction is conventionally supplied by small perforators from the left P1 segment basilar tip, left P2 segment. These segments are normal.
There is also supply from posterior communicators. The posterior communicators are present, reasonable caliber bilaterally.
Therefore likely occlusion of a very small branch vessel, not visible to MR. In the anterior circulation ICAs are flowing, M1 and A1 segments are flowing. Equal peripheral penetration of MCA and ACA branches.
CONCLUSION: Small left thalamic fresh infarct, which correlates very well with the symptoms.
Case Discussion
This case demonstrates the sensitivity of MRI in identifying small, deep ischemic strokes (in this case a thalamic stroke) that may not necessarily be shown on a conventional CT angiogram, as part of a normal stroke protocol.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.