
Presentation
Progressive shortness of breath
Patient Data


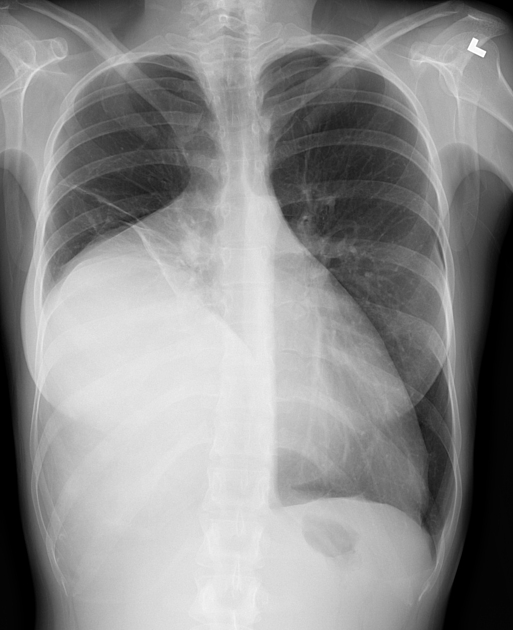
On the frontal radiograph, there is a large mass-like opacity obscuring the right inferior hemidiaphragm, including the right heart border and hemidiaphragm. The left hemithorax is normal.
On the lateral radiograph, the inferior hemithorax is obscured by the mass, including the lower retrosternal clear space. The anterior cardiac border is silhouetted by the mass as well. The right hemidiaphragm is not identified.
Imaging appearances are suggestive of an anterior inferior mediastinal mass.
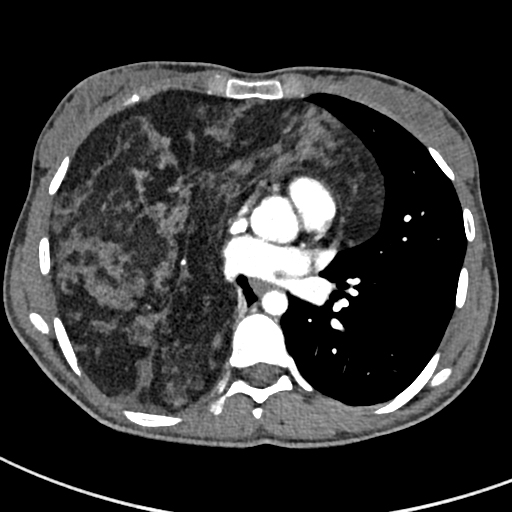
Chest CT with contrast confirms a large right anterior mediastinal mass of predominantly fat attenuation with a 'draped' appearance on either side of the pericardium to reach the diaphragms inferiorly.
There is associated interspersed inhomogeneous and serpiginous, soft tissue attenuation representing thymic tissue.
There are no calcifications and no fat-fluid levels. There are no suspicious mediastinal or hilar lymph nodes.
Case Discussion
Thymolipomas comprise nearly 5% of all neoplasms of thymic origin. They are less common than a mediastinal lipoma of non-thymic origin. There is no sex predilection and the reported age range for these lesions is between 3-56 years, with a mean age of 22 years.
In this case, features suggestive of a thymolipoma are the anterior mediastinal location and the presence of soft tissue attenuation tissue scattered within the macroscopic fat attenuation.
Limited differential diagnoses for fatty mediastinal masses include teratoma, lipoma, and liposarcoma are considered less likely.
Paraneoplastic conditions such as myasthenia gravis, Graves disease and hematological disorders are rarely associated with thymolipoma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.