
Presentation
Gymnastics injury. Landed awkwardly. Now unable to weight-bear. Tenderness at the lateral malleolus. Rule out fracture.
Patient Data



On the AP projection, there is a vertical radiolucency at the midpoint of the tibial epiphysis indicating fracture.
Further fracture extending through the physeal plate (toward the syndesmosis).
On the lateral ankle projection, there is widening at the anterior aspect of the physis, with an oblique fracture extending through the posterior tibial metaphysis.
Large ankle joint effusion.
Imaging features are consistent with triplane fracture (Salter-Harris type-four fracture).
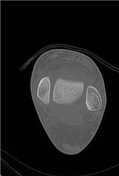




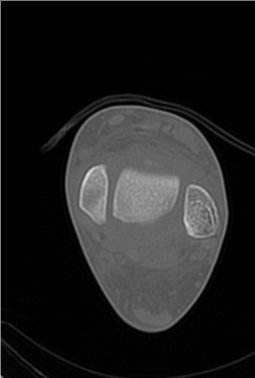
There is a triplane fracture of the distal tibia. The fracture line passes through the metaphysis, physis plate, and epiphysis of the distal tibia and comminuted with the articular surface. There is mild fragmentation of the calcified epiphysis.
An accessory ossicle is seen adjacent to the fibula. An accessory ossicle adjacent to the navicular is seen. The distal tibiofibular joint, ankle joint, subtalar, and tarsal joint articulations are within normal limits.
Case Discussion
Triplane fracture is a type of Salter-Harris type 4 injury and comprises of a vertical fracture through the epiphysis, horizontal fracture through the physis and oblique fracture through the metaphysis.
This type of fracture pattern is most common in young adolescents due to physeal closure at the distal tibia. Typically skeletal growth occurs until 16 years in males and 14 years in females. Physeal closure occurs centrally first, then progresses anteromedially, posterolaterally and finally laterally. This process takes around 18 to 20 months. During this period of incomplete growth, the unfused section is therefore at risk of fracture.
In this case, the patient was treated operatively with two cannulated screws to compress and stabilise fracture.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.