
Presentation
The patient presented with nonspecific lower back pain with no neurological deficits. Initial MRI study performed with follow-up CT and intervention performed.
Patient Data
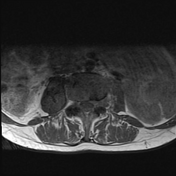

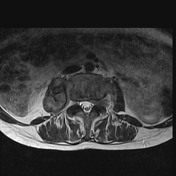

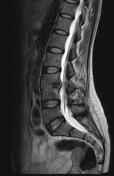
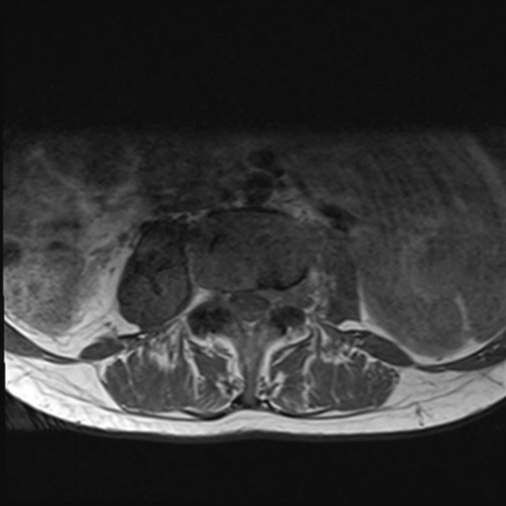
Axial and sagittal T1- and T2-weighted MRI sequences demonstrated spondylodiscitis at the L3-L4 level with disc destruction with loss of intervertebral disc height. Complex fluid collection L3/L4 Extending to right psoas collection. No spinal cord compression.
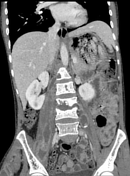
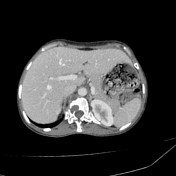
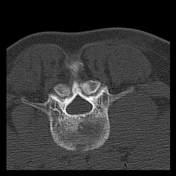

Features consistent with tuberculous (TB) spondylodiscitis, including vertebral body involvement with destruction and spread into the right psoas muscle, forming a psoas abscess. The infection extends further into the right thigh, indicating advanced disease progression. No sagittal series available.
Case Discussion
Initial MRI performed with follow-up CT, percutaneous drain placed, and pus sample confirmed Rifampacin sensitive TB.
This case highlights the critical importance of early diagnosis of tuberculosis (TB) spondylodiscitis to prevent severe complications such as vertebral body destruction and spinal instability. Delayed recognition and treatment can lead to the development of extensive psoas abscesses, as seen bilaterally in this case, with potential further extension into the thigh, increasing morbidity 1.
These abscesses can spread along anatomical planes, causing significant pain, functional impairment, and systemic infection. Early intervention, including appropriate antimicrobial therapy and timely drainage of abscesses, is essential to prevent such extensive complications 2.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.