
Presentation
Left neck mass with dysphagia. Multiple skin café au lait spots.
Patient Data
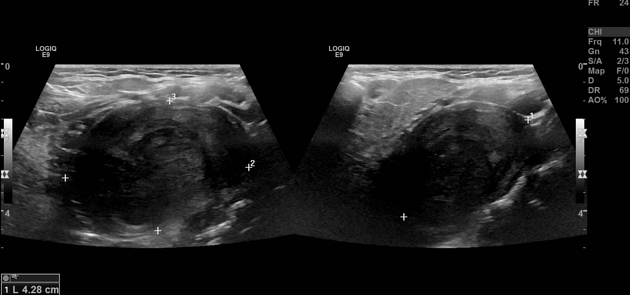
There is a large heterogeneous (mainly hypoechoic) mass lesion with internal vascularity and no internal calcifications, seen just above and deep to the left carotid bifurcation, displacing them anteriorly and anterior to the cervical vertebrae.
Features may suggest a peripheral nerve sheath tumour.
Multiple bilateral cervical lymph nodes that are subcentimetre in the short axis are oval and maintain a fatty hilum.
The thyroid gland showed a pseudo-nodular pattern with normal size and vascularity, with no definite focal lesion. Findings are suggestive of chronic thyroiditis.
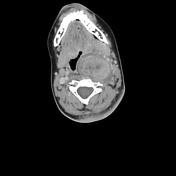

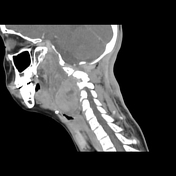

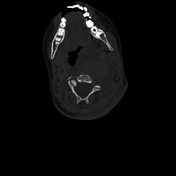
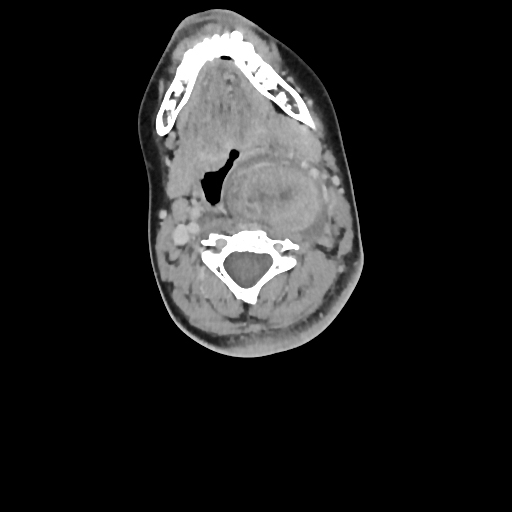
There is a large, relatively well-defined enhancing heterogeneous left neck mass lesion with necrotic changes, likely originating from the left pre-vertebral space extending from C1-C5 levels. This mass encases the odontoid process of C2, displacing the left carotid sheath vessels anterolaterally and deviating the para-pharyngeal space to the right side. It is associated with a hypodense component extending into the left posterolateral neck spaces, insinuating between neck muscles.
A left anterolateral meningocele is noted, arising just anterior to the left jugular foramen, seen posterior to the cervical internal carotid artery.
Radiolucency is seen near the left lambdoid suture (features of neurofibromatosis type 1).
There are no pathologically enlarged cervical lymph nodes bilaterally.
The thyroid gland shows a heterogeneous appearance.

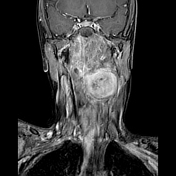
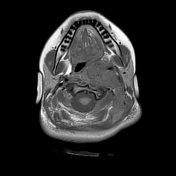
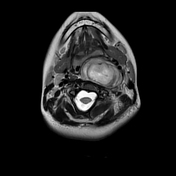
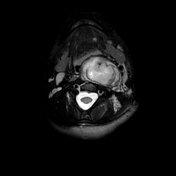
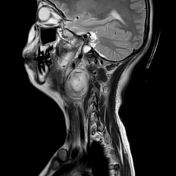



There is a large, relatively well-defined enhancing left neck mass lesion, likely originating from the left pre-vertebral space extending from C1-C4 levels. It appears mainly isointense on T1WI and hyperintense on T2WI.
This mass is seen involving the left longus colli muscle, extending and encasing the odontoid process of C2, displacing the left carotid sheath vessels anterolateral, and deviating the para-pharyngeal space to the right side.
It is associated with a hyperintense component extending into the left posterolateral neck spaces, insinuating between neck muscles.
A left anterolateral meningocele is noted, arising just anterior to the left jugular foramen, seen posterior to the cervical internal carotid artery.
Few high T2 foci are noted in both globi pallidi (FASI).
Histopathology
The patient underwent direct laryngoscopy and a biopsy was taken from the neck mass.
Microscopic evaluation revealed:
Hypocellular proliferation of spindle cells with interspersed collagen bundles and mucin. The spindle cells showed bland cytomorphology. Scattered mast cells were seen.
No necrosis or mitotic activity.
Conclusion: Benign nerve sheath tumour consistent with neurofibroma.
Case Discussion
Neurofibromas are benign nerve sheath tumours of the peripheral nervous system. They affect a single peripheral nerve or multiple nerve bundles (plexiform neurofibromas). These tumours remain benign throughout life and do not become malignant cancers.
Focal areas of signal intensity (FASI) tend to occur in the basal ganglia (often globus pallidus and thalamus), brainstem, cerebellum, and hippocampus in children with neurofibromatosis type 1 (NF1).
The patient is under investigation for the diagnosis of neurofibromatosis type 1 (NF1).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.