
SOLID EPITHELIAL NEOPLASM
- Pancreatic adenocarcinoma: ~90% of all pancreas tumors. Hypoenhancing mass usually near the head, best seen on early arterial phase. Double duct sign.
- Acinar cell carcinoma: Very rare, seen in elderly males. Syndrome of extremely high lipase with fat necrosis (causing subcutaneous nodules), bone infarcts (polyarthralgia), and eosinophilia.
CYSTIC TUMORS: (2) Types, Cystic Epithelial and Endocrine
CYSTIC EPITHELIAL NEOPLASM
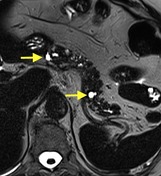
- Serous Cystadenoma: Benign. Seen in elderly women, A conglomerate mass of numerous small cysts, with hyper enhancement. May show a central stellate calcification.
- Mucinous cystic neoplasm: Benign, but w/malignant potential, therefore removed. Either a single cyst or small group of ~6 cysts, in the pancreas body/tail. +Capsule.
- Solid and Papillary Epithelial Neoplasm (SPEN): Low malignant potential, therefore removed. Adolescent and young adult women. Heterogenous, large mass, that is centrally cystic and with enhancing solid peripheral components. Maybe heterogenous throughout secondary hemorrhagic degeneration. +Capsule.
- Intraductal Papillary Mucinous Neoplasm (IPMN): Demographics vary, but classically in elderly men. Cystic mass, or "cluster of grapes" which can be seen communicating with the main duct (main duct IPMN), or communicating with a side duct ("side branch IPMN).
PANCREATIC ENDOCRINE TUMORS
- Generally: Include in your cystic tumor ddx because these become cystic after chronic degeneration. Arterially hyperenhancing, solid/cystic, with calcifications. Tiny tumors present early with symptoms because their hormonely active, large tumors present late b/c are not hormonely active.
- Insulinoma most common > Gastrinoma > Glucagonoma. VIPoma and Somatosatinoma are very rare.





















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.