
GLIAL TUMORS: Glia are support cells that hold neurons in place. Glia meaning "glue" or "clay." Glial cells include: Astrocytes, Oligodendrocytes, Ependymal cells, and Choroid Plexus Cells.
-
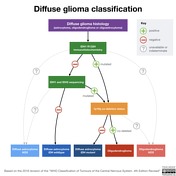
DIFFUSE GLIOMAS CLASSIFICATION:
- Unremarkable IDH genes = Diffuse Astrocytoma IDH Wildtype. Worse px.
- Mutated IDH. Better px -> Next consider 1p/19q Co-deletion.
- Yes they are Co-deleted -> Oligodendroglioma.
- No they are not Co-deleted -> Diffuse astrocytoma IDH Mutant.
- T2-FLAIR Mismatch: Entirely T2 bright, with central area going isointense on FLAIR with a FLAIR bright margin. A mutated IDH tumor that has this mismatch tells you its a IDM Mutated diffuse astrocytoma and not an oligo.
-
ASTROCYTOMAS
- Juvenile Pilocytic Astrocytoma: WHO Grade I. Usually presents in child with a posterior fossa cyst w/enhancing mural nodule.
- Low Grade Diffuse Astrocytoma: WHO Grade II. Infiltrative mass, with blurred GW junctions. Causes gyral swelling. No enhancement. Cannot tell apart from an Anaplastic Astrocytoma.
- Gliomatosis Cerebri: Reclassifed by WHO 2016 as a growth pattern, and a distinct tumor. Invades (2) lobes plus a non-cortical structure (i.e. BG, corpus callosum, brain stem or cerebellum). Diffuse T2 throughout involved brain, no enhancement. Crosses midline to other hemisphere via commisures, corpus callusom, and interthalamic adhesion. Can degenerate to GBM. DDx in immunocompromised: Lymphoma, PML, AIDs encephalopathy.
- Anaplastic Astrocytoma: Many presentations, maybe identical to diffuse low grade astrocytoma w/ill-defined infilitrative non-enhancing mass, or present as a discrete enhancing WM mass. Can degenerate to GBM.
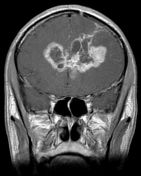
- Glioblastoma (previously called GBM): WHO Grade IV. Most comon adult primary brain tumor; poor px. GBMs come as Primary and Secondary: 1)90% are Primary which are IDH wild-type and have worse px; 2)10% are Secondary (meaning they represent degeneration from a lower grade astrocytic tumor) are seen in older patients, are [IDH mutant +] and have a better px. Higher grade evident by enhancement (confirms angiogenesis), inc'd CHO:NAA ratio, and internal necrosis. Spread via WM tracts, subependymal areas, and CSF.
- OLIGODENDROGLIOMA: WHO Grade II, cortically based, slow growing mass, with little adjacent WM edema, likely chunky calcifications and seen in a young to mid-aged adult. Pre 2016 these were dx'd w/histology alone, but post-2016 WHO grading, these tumors now include several histologic patterns so long as the molecular testing shows [+IDH mutation] and [1p19q co-deletion]. Histologic patterns include: Astrocytomas, Oligodendrogliomas and Oligoastrocytomas.























































 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.