
Presentation
One week history of weakness of the lower extremities and the left upper extremity as well as dysarthria.
Patient Data

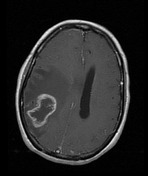

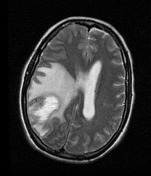

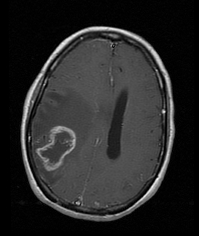
There is a heterogenous mass lesion involving the right parietal cerebral cortex and white matter associated with extensive perilesional vasogenic edema with mass effect. There is also a 12.5 mm right to left subfalcine herniation as well as right uncal herniation.
The mass demonstrates mixed low and intermediate T1. The mass also demonstrates mixed intermediate and high T2 signal intensities and peripheral contrast enhancement. The mass measures 53.5 mm x 38.7mm x 29.8 (AP x CC x Transverse). There is partial effacement of the posterior body and atrium of the right lateral ventricle as well as dilatation of the left lateral ventricle and temporal horn of the right lateral ventricle.
Impression: Right parietal cerebral heterogeneous mass with central necrosis.
Case Discussion
Pathology report
This lesion shows an anaplastic tumor with predominantly a mesenchymal morphology with extensive myxoid change alternating with areas of astrocytic morphology. The neoplastic cells show nuclear pleomorphism and mitotic activity. Endothelial hyperplasia and necrosis are identified. A reticulin stain highlights the mesenchymal component, while an immunostain for GFAP highlights the astrocytic component. The Ki67 proliferation index is approximately 20%. Immunostains are negative for cytokeratins (CAM 5.2), DMA and HMB 45.
CONCLUSION: The morphologic and immunohistochemical features are consistent with the diagnosis of gliosarcoma, WHO Grade IV.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.