


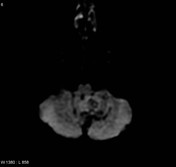

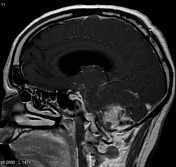
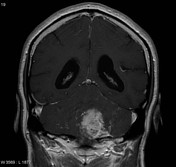


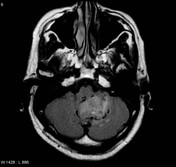
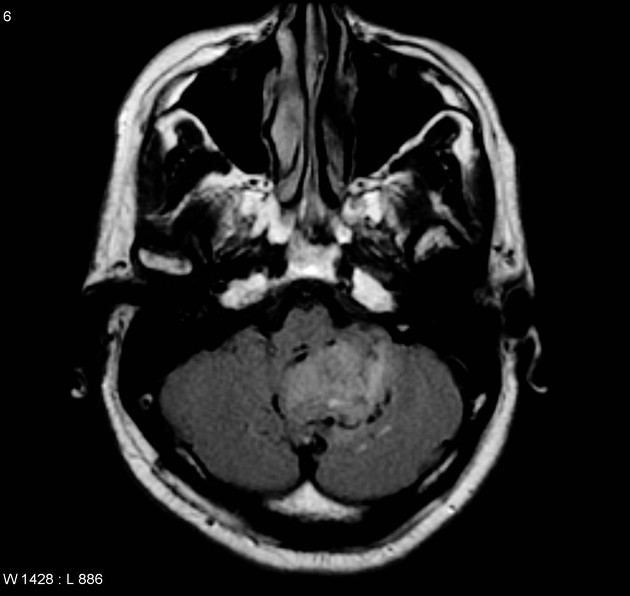
There is a T2 / FLAIR high signal lesion in the left cerebellar hemisphere, exerting positive mass effect on the brain stem and fourth ventricle, causing lateral and third ventricular dilatation (hydrocephalus). The mass is heterogeneously, but avidly enhancing.
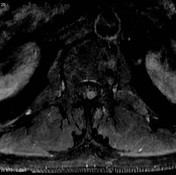
There is an enhancing lesion at the level of first lumbar vertebra, appears to be intradural, extramedullary, most in keeping with drop mets.

Enhancing nodule within the central canal at the level of L1.
Case Discussion
This patient had an initial histology diagnosis of a pilocytic astrocytoma, which did not fit the imaging findings. Review of the entire specimen demonstrated a medulloblastoma with astrocytic components.
Final Diagnosis:
Cerebellum: Primitive neuroectodermal tumor (medulloblastoma) showing areas of glial differentiation. See comment.
Final Diagnosis Comment:
This cerebellar tumor displays predominant features of a primitive neuroectodermal tumor, or medulloblastoma. Areas of astrocytic differentiation are well defined, and relatively distinct from the primitive neuroectodermal component.
Microscopic Description:
Sections show pieces of a primary CNS neoplasm displaying various histologic features. Cerebellar tissue is diffusely infiltrated by a small cell tumor, which is characterized by scanty perinuclear cytoplasm, and round nuclei. Mitotic activity is significantly elevated. Areas of tumor necrosis are seen, and associated vascular neogenesis is observed. The tumor cells permeate diffusely throughout cerebellar tissues, and form no distinct architectural pattern. Homer-Wright rosette formation is suggested within areas of the tumor. The other histologic component, which is distinct from the latter, is astrocytic in appearance and is characterized by larger cells with elongated nuclei and frequently bipolar cellular processes. Cellular cytoplasm is more abundant. Nuclear pleomorphism is variable. Some ganglion-type cells are noted adjacent to the small cell component, which is by far the predominant element in this composite neoplasm. Immunoperoxidase studies confirm immunoreactivity for synaptophysin within the astrocytic areas, and the more primitive component. There is GFAP immunoreactivity within the astrocytic areas. Rare cells display immunoreactivity for smooth muscle actin and desmin. There is variable immunoreactivity for MIB1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.