
Airway invasive aspergillosis, also known as Aspergillus bronchopneumonia or bronchopneumonic aspergillosis, refers to a form of invasive aspergillosis that affects the airways as the major or only feature.
On this page:
Epidemiology
It usually occurs in immunocompromised neutropenic patients, particularly HIV/AIDS patients. Aspergillosis affecting the airways as the major or only feature of the invasive disease is uncommon and is thought to occur in only around 7% of cases of intrathoracic aspergillosis 3.
Clinical presentation
Clinical manifestations can vary and range from an acute tracheobronchitis, to bronchiolitis to bronchopneumonia.
Pathology
It is histologically characterised by the presence of Aspergillus organisms deep to the airway basement membrane 1.
Two morphological forms of invasive aspergillosis of the trachea and bronchi have been described 3:
intraluminal: circumferential and superficial “pseudomembrane” of necrotic tissue, fibrin and hyphae, which may result in airway occlusion
multiple nodular plaques: invades adjacent tissues and may lead to broncho-oesophageal and fatal haemorrhage from bronchoarterial fistulation
Markers (bronchoalveolar lavage)
-
some studies have shown galactomannan (GM) detection in bronchoalveolar lavage fluid (BALF) of
greater than 0.77 in nonneutropenic patients or
GM index of > 1 in patients with AML or myelodysplasia undergoing intensive chemotherapy and patients receiving an allogeneic stem cell transplantation who are in the early engraftment phase, as being suggestive airway invasive aspergillosis.
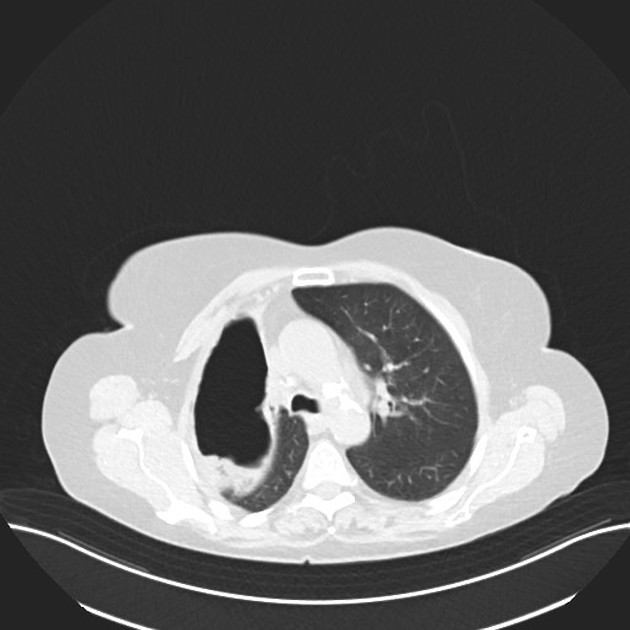
Radiographic features
CT
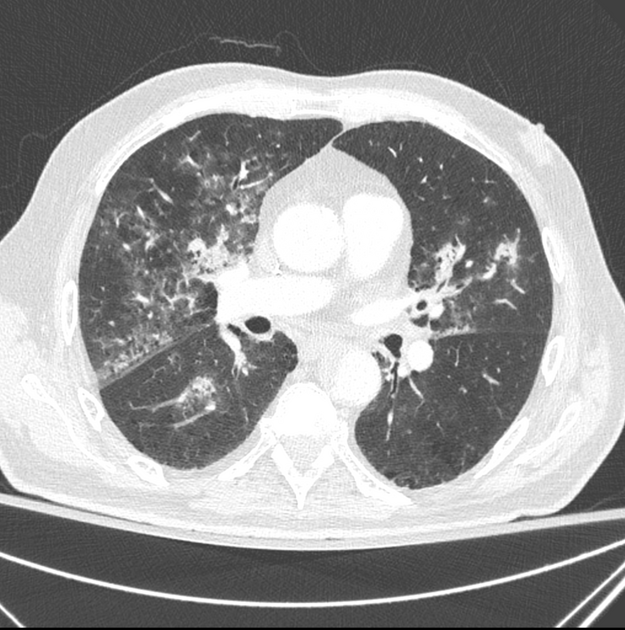
The imaging spectrum is variable, depending on whether is it an obstructive tracheobronchitis, bronchiolitis or bronchopneumonia:
-
obstructive tracheobronchitis due to aspergillosis
most have normal radiographic findings in the acute phase
occasionally, tracheal or bronchial wall thickening may be seen
-
usually seen as centrilobular nodules and branching linear or nodular areas of increased attenuation having a “tree-in-bud” appearance
the centrilobular nodules have a patchy distribution in the lung
-
typically seen as predominantly peribronchial areas of consolidation
rarely, there can be lobar consolidation
it is almost impossible to differentiate Aspergillus bronchopneumonia from bronchopneumonia due to other causes


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.