
Anal atresia, or imperforate anus, refers to a spectrum of anorectal abnormalities ranging from a membranous separation to complete absence of the anus.
On this page:
Epidemiology
The estimated incidence is 1 in 5000 live births.
Associations
There are frequent associations with other congenital abnormalities.
-
other atresias
VACTERL association
caudal regression syndrome: associated sacral agenesis and lower limb hypoplasia
Currarino triad: anorectal malformations with sacral anomalies and presacral mass lesion 6
Clinical presentation
Clinically there is no anal opening and failure to pass meconium.
Pathology
Subtypes can be classified into two broad categories: high (supralevator) or low (infralevator), depending on the location of the atretic portion.
Genetics
Most cases are sporadic, with occasional familial forms.
Radiographic features
Plain radiograph
Abdominal radiograph
can be variable depending on the site of atresia (i.e. high or low), level of meconium impaction and physiological effects such as straining
may show multiple dilated bowel loops with an absence of rectal gas
air within urinary bladder suggests high type 6
calcified meconium in the bowel loops would suggest high type (meconium calcifies due to urine exposure) 6
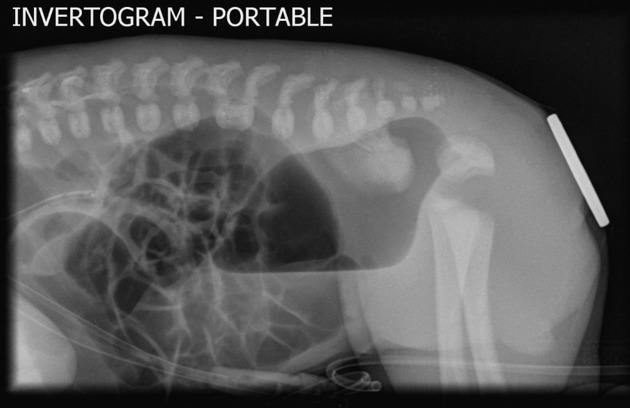
Invertogram
A coin/metal piece is placed over the expected anus and the baby is turned upside down (for a minimum of 3 minutes).
The distance of the gas bubble in the rectum from the metal piece is noted:
>2 cm denotes high type
<2 cm denotes low type
False-positives may occur if the image is taken in the first 24 hours of life or if there is impacted meconium within the distal rectum 6.
For radiographic technique, see invertogram view and prone cross-table lateral view articles.
Fluoroscopy (contrast study)
The fistula is considered low (below the levator ani plane) if it is below the pubococcygeal line and high if above it
Ultrasound
the anus may be seen as an echogenic spot at the level of the perineum and in anal atresia, this echogenic spot may be absent 4. This sign may be appreciated on antenatal sonography as well
may show bowel dilatation
an infracoccygeal or transperineal approach may allow differentiation between high and low subtypes 4
kidneys should be assessed in such patients 6
spinal US can reveal spinal cord lesions like tethering of cord 6
MRI
Can be used pre/post-operatively to study pelvic floor, renal, and spinal abnormalities 6.
Treatment and prognosis
low subtypes are treated with anoplasty
high subtypes are treated with colostomy with subsequent potential repair
Complications
See also
anorectal malformation








 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.