
Anomalous origin of one pulmonary artery from the aorta (AOPA) represents a rare congenital cardiovascular anomaly. One pulmonary artery originates from the aorta and the other from the right ventricular outflow tract 1-3. It more often involves the right pulmonary artery than the left pulmonary artery and is characterized by separate aortic and pulmonary valves 1-4.
On this page:
Terminology
An anomalous origin of one pulmonary artery from the aorta (AOPA) is also known under the term ‘hemitruncus’ although this description is probably inaccurate 1,4.
Epidemiology
An anomalous origin of a pulmonary artery from the aorta is rare accounting for significantly less than 0.5% of congenital heart diseases. The vast majority of cases are diagnosed during infancy. The right pulmonary artery is significantly more commonly involved (80-90%) than the left (10-15%) 2.
Associations
Anomalous origin of one pulmonary artery from the aorta is associated with pulmonary arterial hypertension.
Also, it has been associated with other congenital cardiovascular anomalies in the vast majority of cases (>80-95%) among them 2-5:
aortic arch anomalies
Whereas the anomalous origin of the right pulmonary artery from the aorta (AORPA) was commonly associated with patent ductus arteriosus, the anomalous origin of the left pulmonary artery (AOLPA) was frequently associated with aortic arch anomalies, especially right-sided aortic arch and ventricular septal defects and tetralogy of Fallot 2,3.
Diagnosis
The diagnosis can conveniently be established by cardiac imaging including echocardiography, cardiac CT, cardiac MRI or invasive cardiac angiography 1-4.
Clinical presentation
Clinical symptoms are those of congestive heart failure and include dyspnea and/or tachypnea, recurrent respiratory infections and failure to thrive. Some patients present with hemoptysis.
Pathology
Anomalous origin of one pulmonary artery from the aorta involves a large high-flow and high-pressure post tricuspid left-to-right shunt with complex pathogenesis and different potential embryological causes for the different subtypes 2,3. It is also characterized by the presence of separate aortic and pulmonic valves 3.
Subtypes
The condition can be classified according to the pulmonary artery involved, and into a proximal and distal subtype 2:
anomalous origin of the right pulmonary artery (AORPA): proximal/distal
anomalous origin of the left pulmonary artery (AOLPA): proximal
Radiographic features
The main radiographic feature is the evidence of an anomalous origin of one pulmonary artery from the aorta with no connection to the main pulmonary artery and separate aortic and pulmonic valves.
Plain radiograph
Chest radiographs might display increased pulmonary vascular markings in the lung affected by the AOPA 3,6.
Ultrasound
Echocardiography
Echocardiography can be used as a confirmation tool and
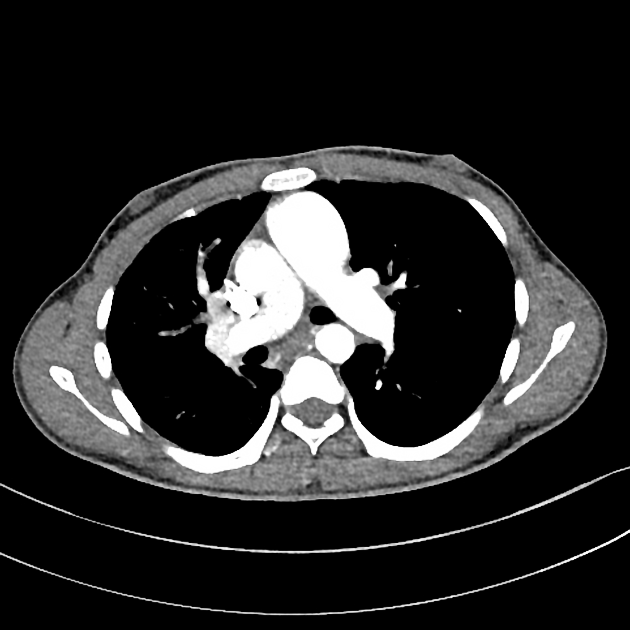
CT
Thoracic CTA is the preferred method for the diagnosis and serves to depict and characterize the anomaly including the exact location of the origin 2,3,7,8.
MRI
Cardiac MRI can clarify anatomy employing traditional black-blood sequences 4 or MRA and might provide additional information with 2D and 4D flow measurements.
Angiography (DSA)
Cardiac catheterization can be used to delineate the anomaly and to measure pulmonary artery pressure and pulmonary vascular resistance 5,6.
Radiology report
The radiology report should include a description of the following 2:
the condition and type
-
location of origin from the aorta
proximal/distal
ipsilateral lateral/posterolateral, contralateral posterolateral, posterior
descending aorta
associated congenital cardiovascular anomalies
Treatment and prognosis
Anomalous origin of one pulmonary artery has a high mortality rate of up to 70% in patients who have not undergone surgical repair during the first year of age 2. That is why surgical intervention is often required already during perinatal period 7,8. Surgical approaches that have been described include the following 7:
direct implantation with or without patch augmentation
use of interposition graft conduit
different flap techniques either from the aorta the main pulmonary artery or both
History and etymology
The abnormal communication of one pulmonary artery with the aorta has been first described by the German military doctor Oscar Fraentzel in 1868 4-8.
Differential diagnosis
truncus arteriosus: common single truncal valve
discontinuous pulmonary arteries


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.