
Birt-Hogg-Dubé syndrome (BHDS), also known as folliculin gene-associated syndrome, is a multi-system disease characterised by:
cutaneous manifestations, typically fibrofolliculomas
multiple lung cysts and spontaneous pneumothoraces
increased risk of renal tumours in some families, typically chromophobe oncocytomas and chromophobe carcinomas
On this page:
Epidemiology
Birt-Hogg-Dubé syndrome is rare but likely underdiagnosed. It may be diagnosed incidentally after a CT scan, dermatological review or a spontaneous pneumothorax. Men and women are equally affected as this is an autosomal dominant disorder. A family history of pneumothorax may be described.
Diagnosis
The diagnosis of BHDS is established on identifying one major or two minor criteria 16.
Major criterion:
five adult-onset fibrofolliculomas
pathogenic FLCN germline mutation
Minor criteria:
typical lung cysts with no other explanation
multifocal/bilateral renal cancer before the age of 50 years
renal cancer of mixed chromophobe and oncocytic histology
first-degree relative with Birt-Hogg-Dubé syndrome
Clinical presentation
-
skin lesions
develop in approximately 80% and manifest in the third and fourth decades and progress over time
fibrofolliculomas are the characteristic lesion, typically seen in the midface
other skin lesions include trichodiscomas and acrochordons (skin tags)
-
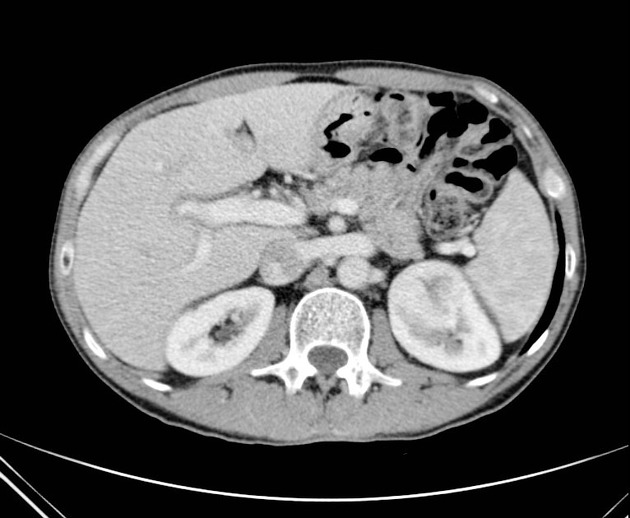
renal cancer
seven-fold increased risk of malignancy
-
unusual histological forms of renal cancer should prompt a search for other features of Birt-Hogg-Dubé syndrome, most often chromophobe oncocytomas and/or chromophobe carcinomas
chromophobe oncocytomas (50%), chromophobe carcinomas (34%), clear cell carcinomas (9%), oncocytomas (5%), papillary renal cell cancers (2%)
tumours are frequently bilateral, multifocal, and slow-growing 13
-
lung cysts
develop in early or mid-adulthood, predating renal cancer
aside from a 50-fold increase in pneumothorax, they are usually asymptomatic
when manifesting, pneumothorax can be recurrent and even bilateral, risk increases with cyst volume and volume changes associated with activities such as flying and diving
Pathology
Folliculin is thought to be an oncogene suppressor protein which may affect proteolytic metalloproteinase enzymes leading to lung matrix breakdown, tissue destruction and cyst formation. However, the exact function of folliculin is unknown 13.
Genetics
Deletion mutation in the folliculin (FLCN) gene (17p11.2) with autosomal dominant inheritance. At least 142 unique DNA mutations of the FLCN gene have been implicated in the pathogenesis of Birt-Hogg-Dubé syndrome, which would explain the variable features in different families 13.
Radiographic features
CT
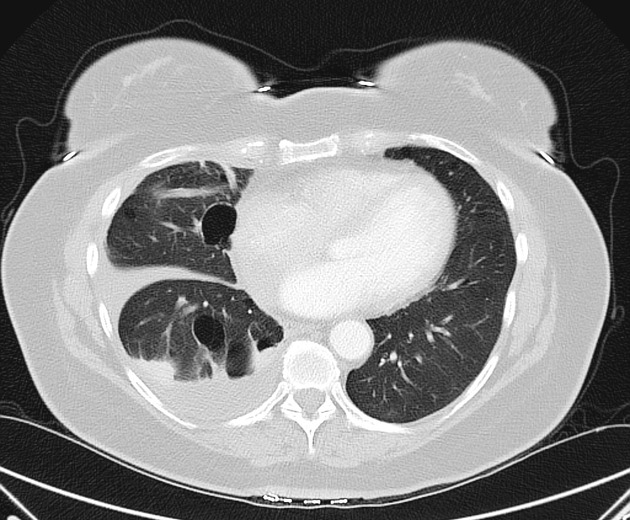
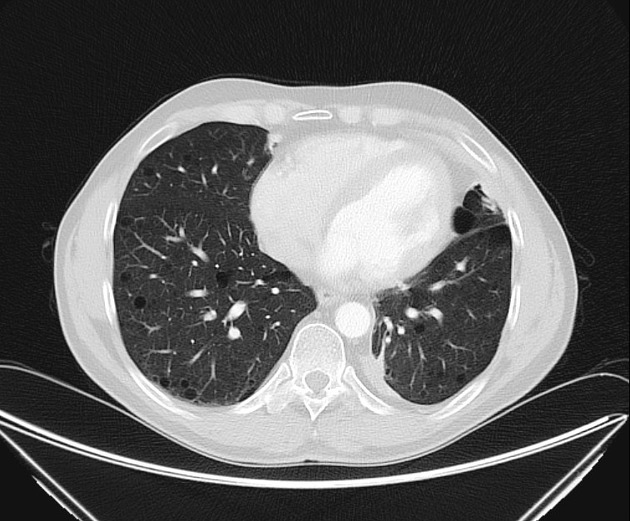
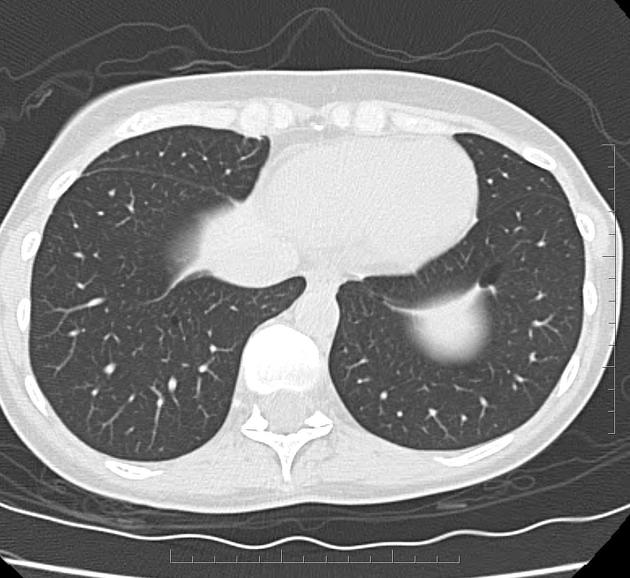
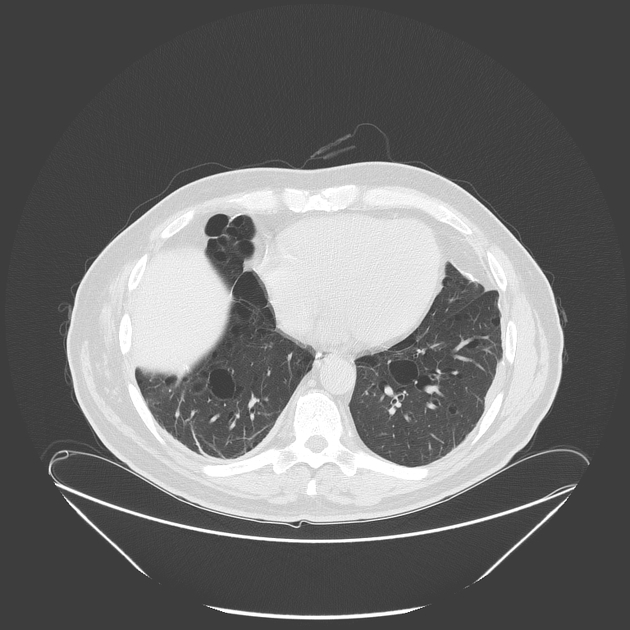
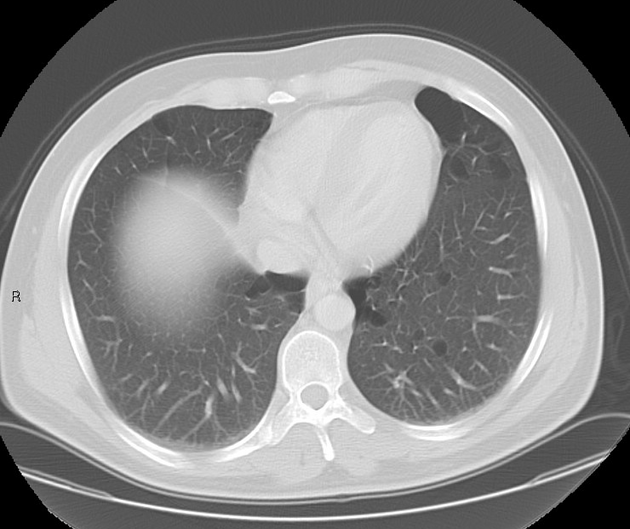
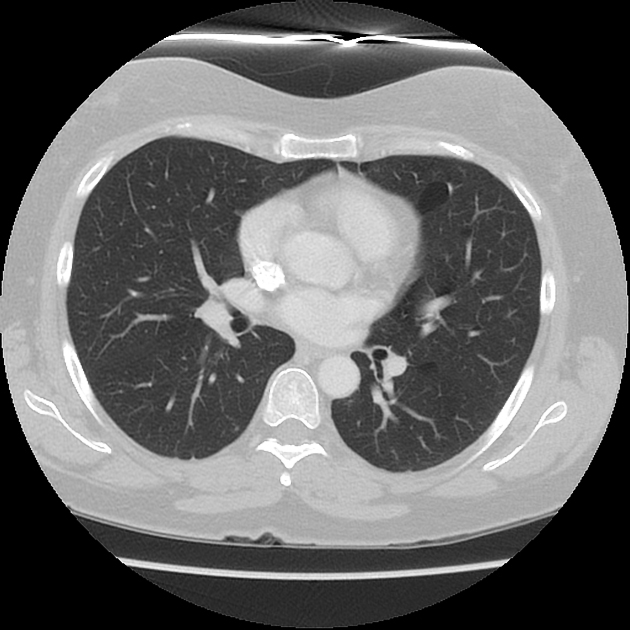
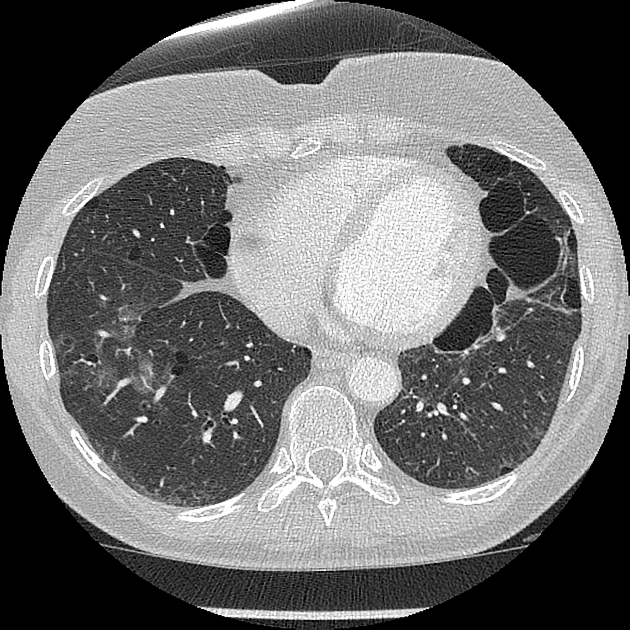
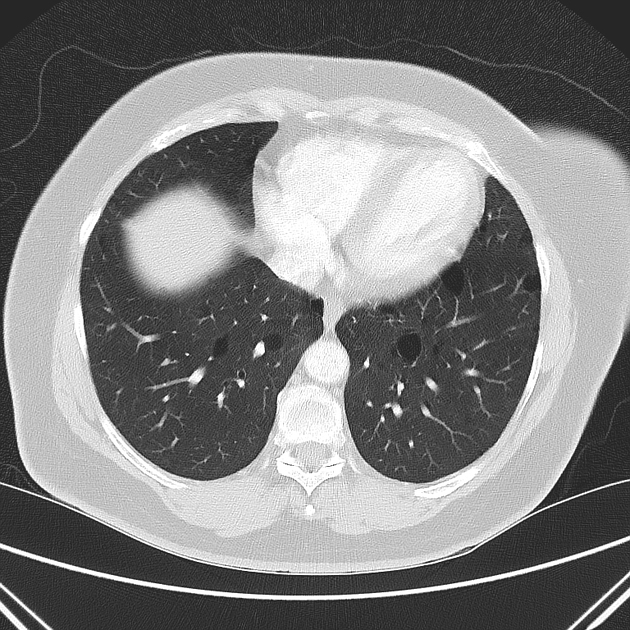
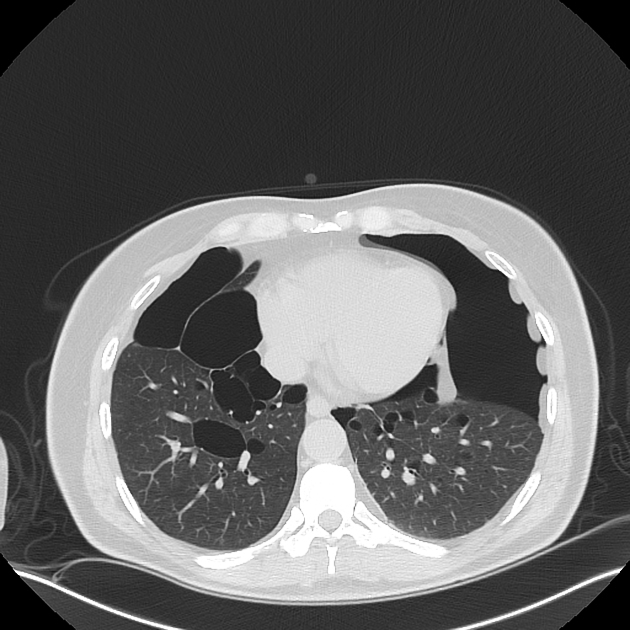
Lung cysts typically develop in early adulthood and have the following characteristics:
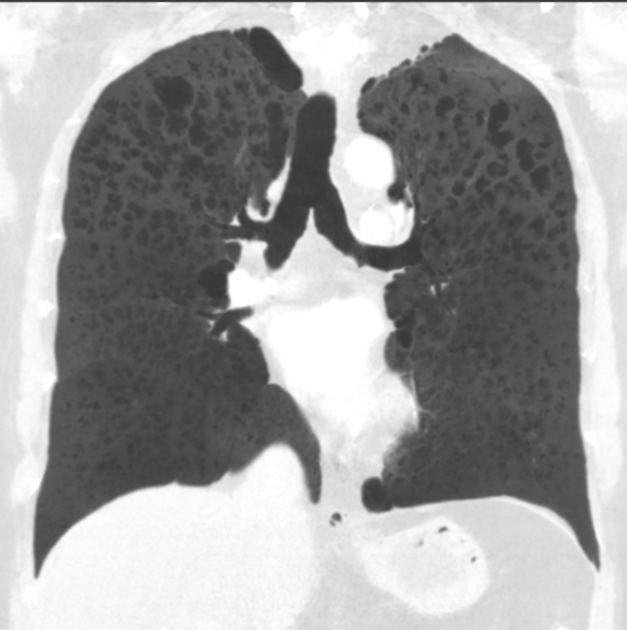
multiple lower zone predominant and bilateral
predilection for subpleural lung including paramediastinal and perifissural location
adjacent to interlobular septa, arteries and veins
thin-walled, variable in size, round or elongated, sometimes multilobulated or multiseptate 13
cysts adjoining the pleura may have a relatively narrow pleural base
cyst rupture may cause pneumothorax, pneumomediastinum or pneumopericardium
Treatment and prognosis
General recommendations include:
genetic testing and counselling
screening of family members
smoking avoidance
Regarding renal cancer:
renal cancer surveillance, initially by MRI, followed by MRI or CT 17 every 1-3 years.
renal cancer prognosis depends on histology
Regarding pneumothoraces and lung disease:
early ipsilateral VATS pleurodesis is recommended after a single pneumothorax
contralateral pleurodesis is usually not required
History and etymology
It is named after Canadian physicians Arthur R Birt (dermatologist), Georgina R Hogg (pathologist) and William James Dubé (internist) who published their findings in 1978 7.
Differential diagnosis
Other causes of cystic lung disease or focal hyperlucencies:
-
lymphangioleiomyomatosis (LAM)
scattered distribution, i.e. no spared areas
absence of sub-pleural cysts along fissures
underlying TSC gene mutations occur in both tuberous sclerosis and sporadic LAM (cysts develop in women during their child-bearing years)
renal angiomyolipomas or other LAM-associated features
-
pulmonary Langerhans cell histiocytosis
upper zone predominant and bronchocentric cavitating nodules, branching or irregular cysts
spares costophrenic and costomediastinal angles
typically a disease of young adult smokers, especially men
-
Sjögren syndrome 15:
perivascular cysts containing soft-tissue strands or vessels
ground glass opacity
consolidation
tree in bud opacities
lymphoma
-
light chain deposition disease
perivascular cysts identical to Sjogren syndrome
nodules and lymphadenopathy
older adult with a plasma cell dyscrasia (e.g. multiple myeloma) and renal failure
desquamative interstitial pneumonia, pneumatocoeles, cystic pulmonary metastases, alpha 1 antitrypsin deficiency, inherited connective tissue disease such as Marfan syndrome, and neurofibromatosis type 1 are less likely to be confused with Birt-Hogg-Dubé syndrome
Practical points
lung MinIPs help to identify lung cysts and their distribution: they are more sensitive than MPRs and are especially useful when screening young adults in whom small cysts can be hard to detect
quantitative CT ‘emphysema’ software for total cyst volume measurement, distribution and monitoring


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}