
Chronic periaortitis is an inflammatory condition typically involving the infrarenal abdominal aorta. It is a rare disease, usually occurring in middle-aged men.
On this page:
Epidemiology
Clinical presentation
Common symptoms include dull, diffuse back/abdominal/flank pain (80%), with other symptoms including fever, weight loss, anorexia, vomiting, malaise, claudication, testicular pain, and/or renal colic.
Pathology
Chronic periaortitis encompasses several conditions 4:
isolated periaortitis: non-aneurysmal form of chronic periaortitis; less frequently encountered
Etiology
Chronic periaortits is considered idiopathic, although not should be made that retroperitoneal fibrosis can be secondary to many conditions 4.
The major pathogenetic process leading to chronic periaortitis is inflammation, caused by advanced atherosclerosis. Lymphocyte populations, periaortic inflammation and fibrosis have been demonstrated in histologic specimens of IRF and IAAA.
Autoimmunity to several components (oxidized-low density lipoproteins and ceroid) of atherosclerotic plaque has been proposed as the antigenic stimulus in the initiation of the inflammatory process.
Associations
The association of periaortitis with various autoimmune diseases has been reported, supporting the concept of autoimmunity. Periaortitis can be seen with:
Markers
Elevated ESR is seen in 80-90% of patients.
Radiographic features
Ultrasound
retroperitoneal fibrosis may be defined as hypoechoic or anechoic
the mass surrounding the aorta is usually well-demarcated but irregularly contoured
varying degrees of hydronephrosis and hydroureter may result
comprehensive evaluation of the prevertebral and paravertebral lumbar spine is essential
the overall sensitivity of sonography is poor
CT
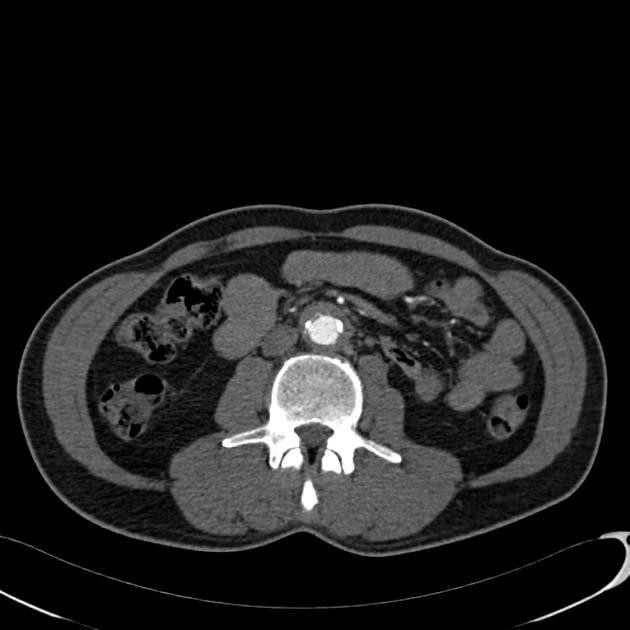
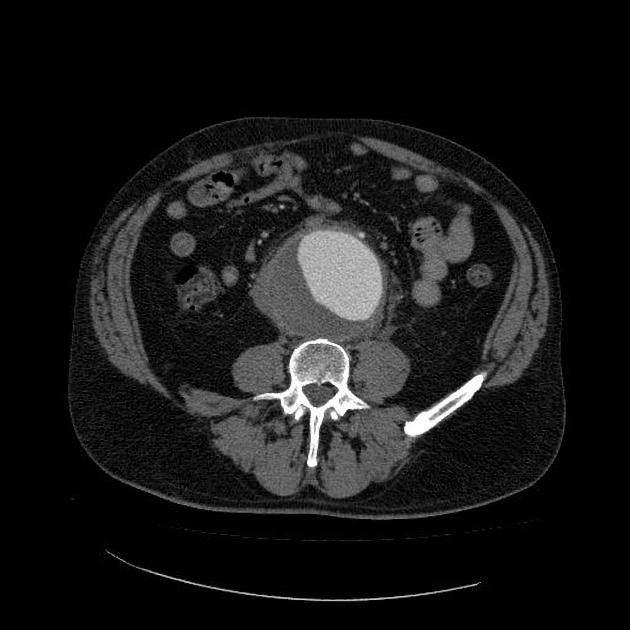
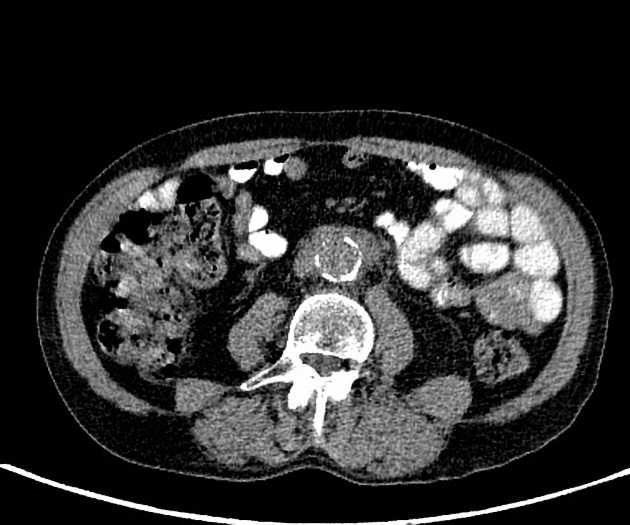
The definitive diagnostic test is contrast-enhanced CT scanning or MRI. Both CT and MRI typically show a periaortic soft tissue mass as a rind of abnormal tissue around the aorta, with a varying extent of spread.
in IAAA the aorta is aneurysmal
in isolated periaortitis, the aorta is not aneurysmal and surrounded by a mantle of soft-tissue density
in IRF, there is usually entrapment of one or both ureters
fibrosis often manifests as a paraspinal, well-demarcated but irregular retroperitoneal mass, isodense to surrounding muscle
-
with CE-CT the periaortic mass usually shows varying degree of enhancement; the degree of enhancement correlates with the activity of the fibrotic process
in acute stages, avid enhancement is seen, with an increase of 20-60HU
in chronic disease, little or no enhancement may be seen
in approximately 1/3 of patients with proven retroperitoneal fibrosis, no abnormality is seen
in malignancy the fibrosis has a tendency to be larger and bulkier; the sensitivity and specificity of morphologic features are rather poor
CT-guided biopsy is usually adequate to exclude malignancy in IRF, occasionally multiple deep biopsies may be required
MRI
periaortitis typically hypointense on T1 and hyperintense on T2
with gadolinium-enhanced MRI, the inflammatory cuff enhances homogeneously
FDG-PET
PET scan and PET-CT with 18F-fluorodeoxyglucose (FDG) is a reliable tool for assessing the metabolic activity of the mass: in early inflammatory stages the uptake is avid, in the late fibrotic stage there might be no uptake.
It is also useful to detect other sites of inflammation and disclosing infectious or neoplastic lesions to which periaortitis can be secondary or associated with.
Treatment and prognosis
Treatment
Steroids have been used along with surgery with good results.
Medical
steroids are usually effective in chronic periaortitis but their role remains somewhat controversial. There is no accepted standard for dose and duration of steroid treatment
immunosuppressive drugs such as Azathioprine and Methotrexate have been used effectively as steroid-sparing agents and in patients unresponsive to steroids alone.
Cyclophosphamide may be useful in severe cases (if vasculitis is present)
Surgical
ureterolysis with lateral transposition of the ureters and wrapping with omentum is the procedure of choice in patients with hydronephrosis in IRF
ureteral stents are also used
operative repair of an aneurysm is the definitive treatment for IAAA. Surgery is performed when the diameter of the aorta is >5 cm
Prognosis
The prognosis for patients with benign retroperitoneal fibrosis is considered to be good. In most instances IRF does not lead to long-term morbidity. Malignant retroperitoneal fibrosis has a mean survival of 3-6 months.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.