
Cryptogenic organising pneumonia (COP) is a disease of unknown aetiology characterised on imaging by multifocal ground glass opacifications and/or consolidation. A wide variety of infectious as well as noninfectious causes may result in a similar histologic pattern.
On this page:
Terminology
Organising pneumonia (OP) is a histological pattern of alveolar inflammation with varied aetiology (including pulmonary infection). The idiopathic form of OP is called cryptogenic organising pneumonia (COP) and it belongs to the idiopathic interstitial pneumonias (IIPs).
COP was previously termed bronchiolitis obliterans organising pneumonia (BOOP), not to be confused with bronchiolitis obliterans 8.
Epidemiology
The presentation is commonest in the 55-60 years age group.
Clinical presentation
Patients present with a short history (i.e. less than ~2 months) of breathlessness, non-productive cough, weight loss, malaise and fever. There is no association with smoking.
Pathology
In addition to the alveolar inflammatory changes found with regular pneumonia, there is also the involvement of the bronchioles.
Histologically, it is characterised by mild chronic patchy interstitial inflammation without fibrosis and the presence of buds of granulation tissue made of mononuclear cells, foamy macrophages, and fibrous tissue (Masson bodies) in the distal airspaces which may cause secondary bronchiolar occlusion due to extension of the inflammatory process. Hence, the reason for being previously termed bronchiolitis obliterans organising pneumonia (BOOP).
Radiographic features
Plain radiograph
-
consolidation
unilateral or bilateral patchy areas (most common finding 3): often migratory
can affect all lung zones
usually peripheral, subpleural, peribronchovascular 2
-
nodules
foci of granulation tissue up to 1 cm
may mimic neoplasm if >5 cm in size
may be numerous in immunocompromised patients
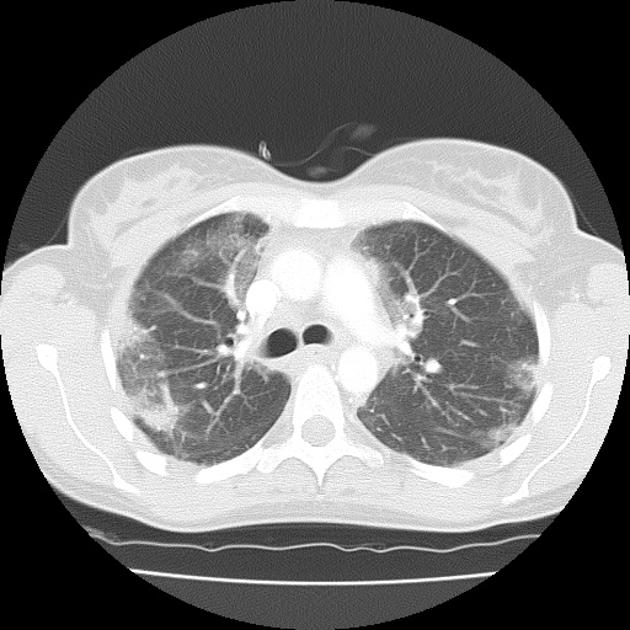
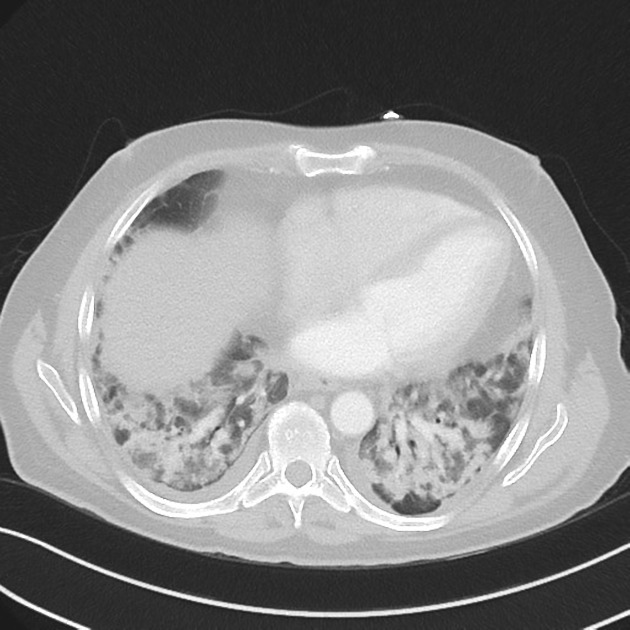
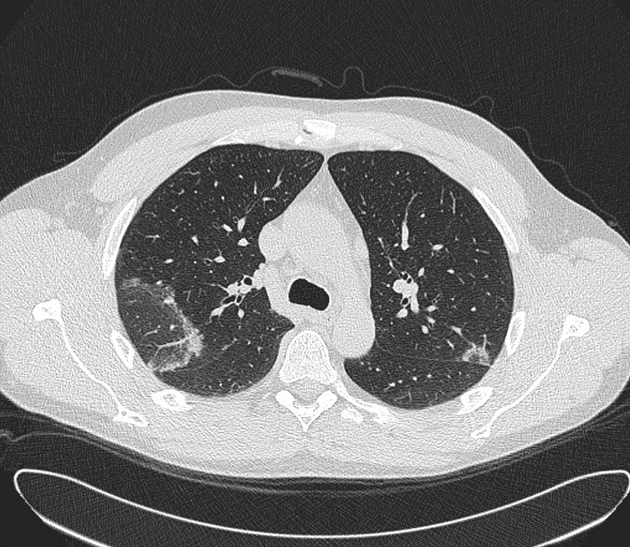
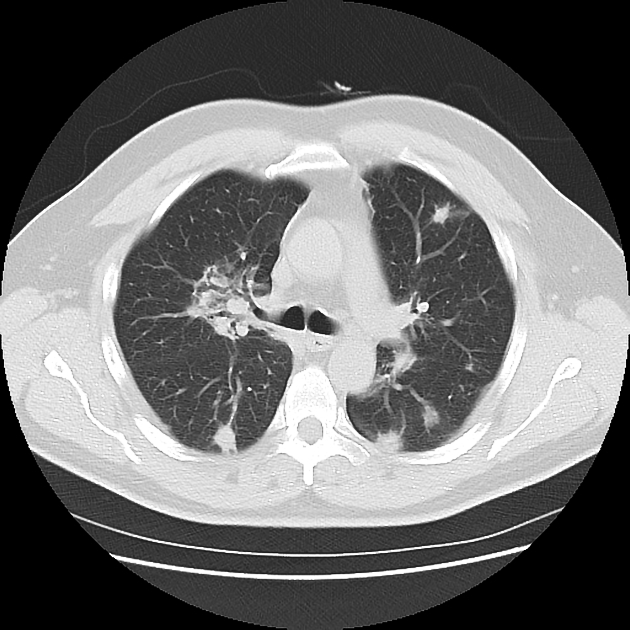
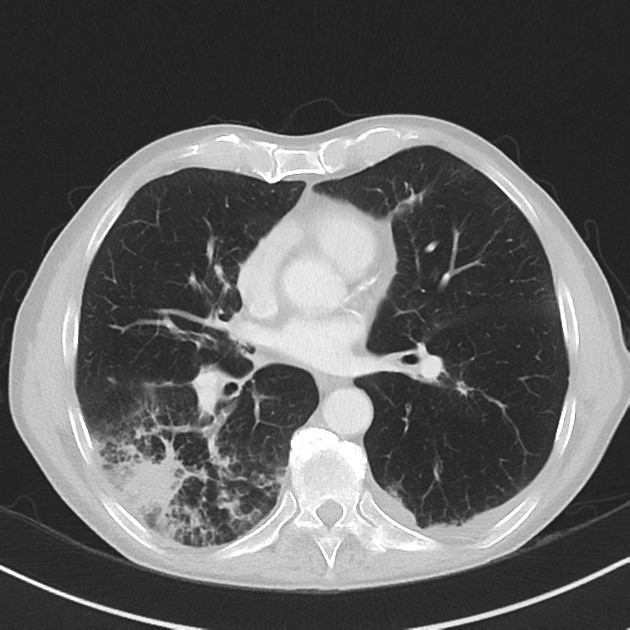
CT
The most common HRCT features include 6:
patchy consolidation with a predominantly subpleural and/or peribronchial distribution
small, ill-defined peribronchial or peribronchiolar nodules
large nodules or masses
bronchial wall thickening or dilatation in the abnormal lung regions
-
a perilobular pattern with ill-defined linear opacities that are thicker than the thickened interlobular septa and have an arcade or polygonal appearance
arcade-like sign of perilobular fibrosis describes an arch pattern in more than half of the patient with COP 13
The reverse halo sign (atoll sign) is considered to be highly specific, although only seen in ~20% of patients with COP 5.
Hilar and mediastinal lymphadenopathy is typically absent 15.
Treatment and prognosis
Corticosteroids have been widely used, and most patients recover completely 3-4.
History and etymology
Cryptogenic organising pneumonia was first described by Davison and colleagues in 1983.
Differential diagnosis
On a radiograph consider:
differential for peripheral consolidation: reverse bat wing opacities
differential for bilateral airspace opacities
On CT consider:
adenocarcinoma in situ or minimally invasive (formerly bronchoalveolar carcinoma)
chronic eosinophilic pneumonia (for a subpleural consolidative pattern)





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.