Cytotoxic lesions of the corpus callosum (CLOCCs)
Updates to Synonym Attributes
Updates to Article Attributes
Transient lesions of the splenium of corpus callosum, also known as mild encephalitis/encephalopathy with a reversible isolated SCC lesion (MERS), are occasionally encountered on MRI studies and may be due to a number of underlying aetiologies.
Clinical presentation
Unlike other causes of splenium of corpus callosum (SCC) lesions, the small transient lesions of the splenium seen in epilepsy and antiepileptic drug cessation use do not demonstrate convincing signs or symptoms of hemispheric disconnection, such as pseudo-neglect, alien hand syndrome, apraxia of the left hand, agraphia, alexia, and visual apraxias 4.
Pathology
Aeitiologies include 1-5:
- epilepsy
- seizures: focal lesions have been described after focal status epilepticus and unusually after single seizures and were explained as focal brain oedema.
- antiepileptic drug usage and sudden cessation
- demyelination
- posterior reversible encephalopathy syndrome (PRES)
- Marchiafava-Bignami disease
- diffuse axonal injury (DAI)
- AIDS dementia complex
- infections
- viral: influenza, measles, herpes, mumps, adenovirus, varicella zoster, rotavirus and HIV
- bacterial: salmonella, Legionnaires disease,
- mycobacterial: tuberculous meningitis
- hypoglycemia
-
hemolytichaemolytic-uremic syndrome with encephalopathy
Radiographic features
Transient lesions of splenium are only really appreciable on MRI where they have two distinct patterns 4:
- well circumscribed, small, oval lesions in the midline within the substance of the corpus callosum
- more extensive ill defined irregular lesions extending throughout the splenium and into the adjacent hemispheres (boomerang sign)
The smaller well circumscribed lesions is the typical lesion seen in the setting of seizures/cessation of anitepileptic medication, whereas the larger lesion is more typical of other aetiologies.
MRI
These lesions tend to demonstrate the following signal characteristics 4:
- T1: hypointense
- T2: hyperintense
- DWI/ADC: restricted diffusion
- T1 C+: no enhancement
Studies have shown that patients recover completely on MRI studies within 1 month, mostly within 1 week following the neurologic recovery 7.
Treatment and prognosis
The prognosis generally depends on the underlying cause, but in the setting of epilepsy or antiepilepic drug related lesions it is very good.
-<li>viral: influenza, measles, herpes, <a title="Mumps" href="/articles/mumps">mumps</a>, adenovirus, varicella zoster, rotavirus and <a href="/articles/hivaids">HIV</a>- +<li>viral: influenza, measles, herpes, <a href="/articles/mumps">mumps</a>, adenovirus, varicella zoster, rotavirus and <a href="/articles/hivaids">HIV</a>
-<li>hemolytic-uremic syndrome with encephalopathy</li>- +<li>haemolytic-uremic syndrome with encephalopathy</li>
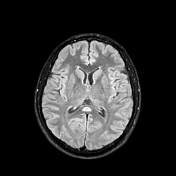
Image 10 MRI (FLAIR) ( create )