
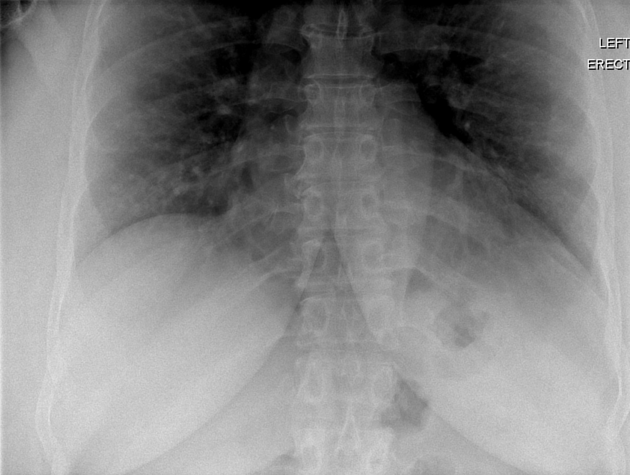
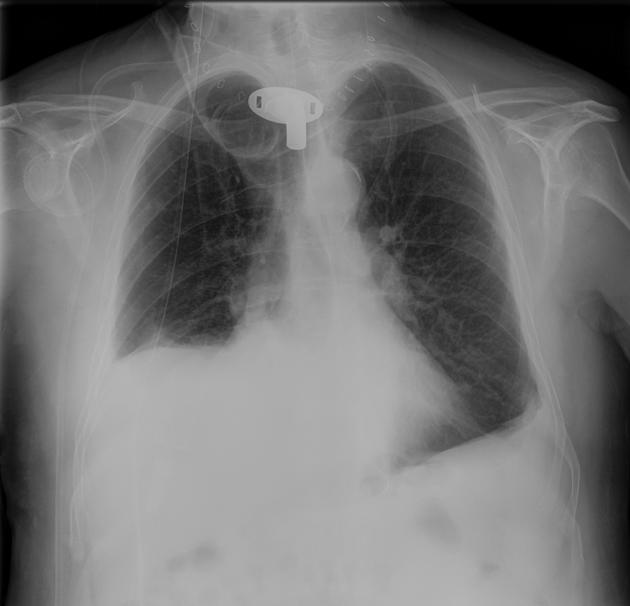
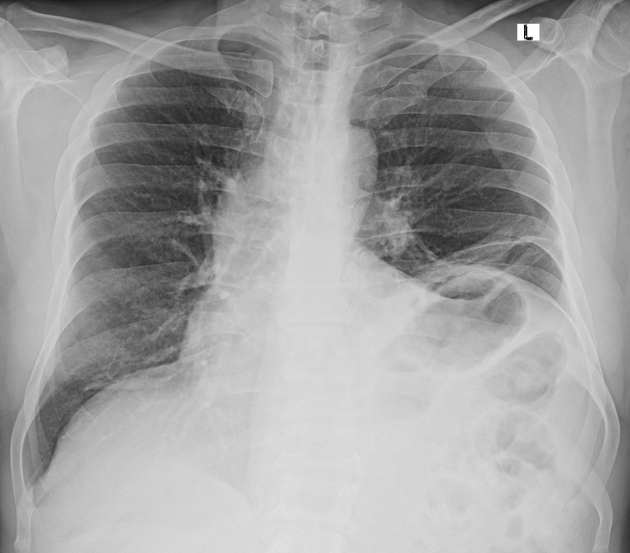
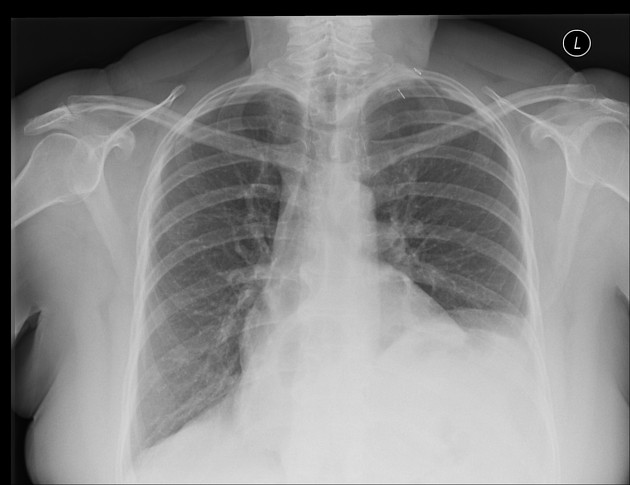
Diaphragmatic paralysis, diaphragmatic paresis or diaphragmatic palsy may be first suspected when a newly elevated hemidiaphragm is seen on a chest radiograph. Bilateral paralysis is far more serious but often overlooked because both hemidiaphragms are elevated; the average delay to diagnosis is 2 years.
On this page:
Clinical presentation
The diaphragm is the primary muscle of ventilation. Unilateral weakness or paralysis increases the work required to breathe and reduces respiratory reserve but may be asymptomatic in the absence of lung disease or abdominal distension. Bilateral paralysis however may require non-invasive nocturnal positive pressure ventilation.
In the erect position the abdominal contents move downwards under the influence of gravity and the position of the diaphragm is correspondingly more inferior. Contraction of the abdominal muscles can aid expiration by elevating the diaphragm above the resting level. Subsequent relaxation allows passive inferior diaphragmatic motion thereby increasing the inspired volume and mimicking normal diaphragmatic contraction. In the supine position this effect is minimised as the abdominal contents press upwards on the diaphragm which consequently lies more superiorly. Patients may present with orthopnoea.
Most cases of bilateral diaphragmatic paralysis (BDP) are idiopathic, and the diagnosis may be made when a ventilated patient cannot be weaned but the more common scenario is a patient with orthopnoea, sleep disturbance, daytime somnolence, morning headaches and anxiety. Thoracic muscle tone is lost during rapid-eye-movement sleep 15 exacerbating hypercapnia and causing hypoxaemia. Dyspnoea when immersed in water is unique to BDP. Both hemidiaphragms are elevated on CXR and the lungs demonstrate atelectasis, a common scenario which can affect anyone with a large abdomen. Diagnosis is typically delayed for around 2 years but is readily apparent if oesophageal and gastric pressure measurements are taken. In BDP thoracic and abdominal pressures are equal and maximal inspiratory pressure is reduced 16.
Pathology
Aetiology
Paralysis may be unilateral or bilateral depending on the cause. Around 70% of cases are idiopathic. Known causes are as follows:
Central nervous system:
cerebral hypoventilation syndrome (Ondine’s curse)
cervical spondylosis
Peripheral nervous system
idiopathic neuralgic amyotrophy
diabetic neuropathy
Phrenic nerve dysfunction
cardiac surgery 7: hypothermia injury and stretch injury
radiofrequency ablation for atrial fibrillation 17
interscalene block for shoulder surgery 12,13
blunt trauma
compression by tumour, aneurysm or goitre
post-viral neuropathy
idiopathic neuropathy
cervical manipulation
Myopathies
malnutrition, vitamin B6 and B12 deficiency
idiopathic myopathy
Radiographic features
Plain radiograph
Normally the right dome of the diaphragm is higher that the left, but there is considerable normal variation. Comparison with prior radiographs helps to identify a change in position.
Fluoroscopy
Normal respiration requires synchronised action of the following:
lung-apposed rib cage (inspiratory and expiratory)
diaphragm plus abdomen-apposed rib cage (inspiratory)
abdomen (expiratory) 18
Unbalanced activity can cause paradoxical motion of one or two compartments and this may explain some of the unexpected fluoroscopic findings.
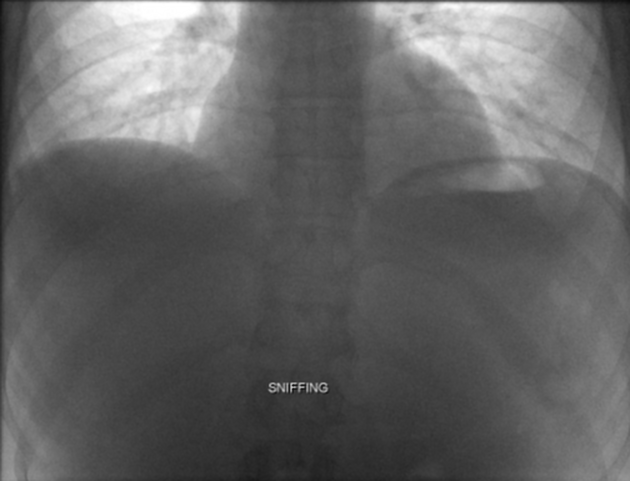
Fluoroscopic examination of the diaphragm ("sniff test") is useful in diagnosing diaphragmatic paralysis. In normal individuals, both hemidiaphragms typically descend with inspiration. In cases of unilateral diaphragmatic paralysis, the affected side may demonstrate paradoxical upward motion. There is considerable normal variation however depending on the contribution of thoracic, diaphragmatic and abdominal breathing; some normal people will demonstrate paradoxical motion of the anterior or the entire diaphragm. Also, in the erect position the abdominal musculature can work to achieve a normal result in the erect position. This effect is minimised in the recumbent position 14.
The diagnosis of BDP can be difficult as there is no normal hemidiaphragm for comparison. Moreover, the cephalad motion of the ribs can give an illusion of diaphragmatic descent. A fixed object should be used to assess diaphragmatic motion.
Ultrasound
Ultrasound is a good substitute for fluoroscopy and can be performed at the bedside with the patient lying flat if they can breathe in this position.
It is easier to evaluate children with ultrasound and avoids radiation risk. Real-time ultrasound is performed in the axial plane to compare the two hemidiaphragms simultaneously. Additional coronal or sagittal M-mode can help quantify the degree of movement of each individual hemidiaphragm. Diagnostic criteria in children include paradoxical movement, excursion of less than 4 mm and a difference >50% between the excursion of one hemidiaphragm compared to the other.
In an adult patient diaphragmatic motion should be >1 cm when observing diaphragmatic craniocaudal excursion in the mid-clavicular line 8. The ability to apply this information and predict the success of weaning a patient from mechanical ventilation tends to be more robust when one measures the contractile nature of the diaphragmatic muscle itself. Medial angulation from a sagittal transducer position in the mid-axillary line allows visualisation of the striated, mixed echogenicity band just cephalad to the liver. After placing an M-mode line, one may pause the recording and measure the end-expiratory and end-inspiratory figures, the latter of which should be larger, and calculate a diaphragmatic thickening fraction; values above 30%, indicating no sonographic diaphragmatic dysfunction, have been found to be 71% specific for extubation success 9.
The thickening fraction of the intercostal muscles as an index of diaphragmatic dysfunction and the use of accessory muscles has a linear, negative relationship with the calculated thickening index of the diaphragm, although insufficient evidence exists to advocate its routine use at this time. Intercostal thickening fractions >8% have, thus far, been deemed pathologic 10.
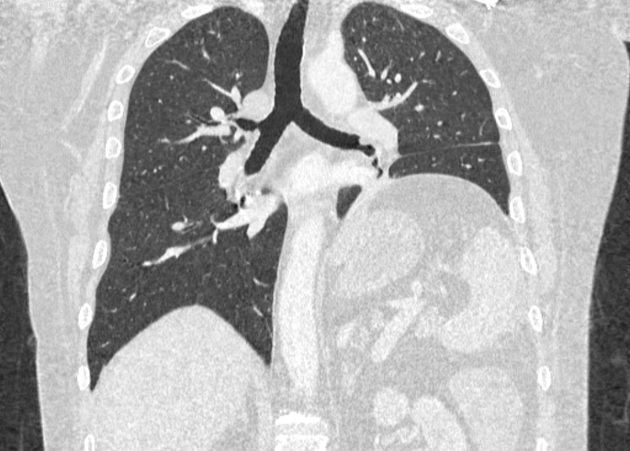
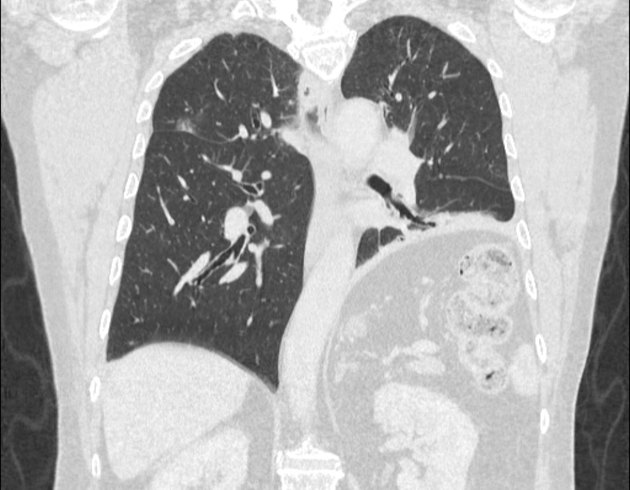
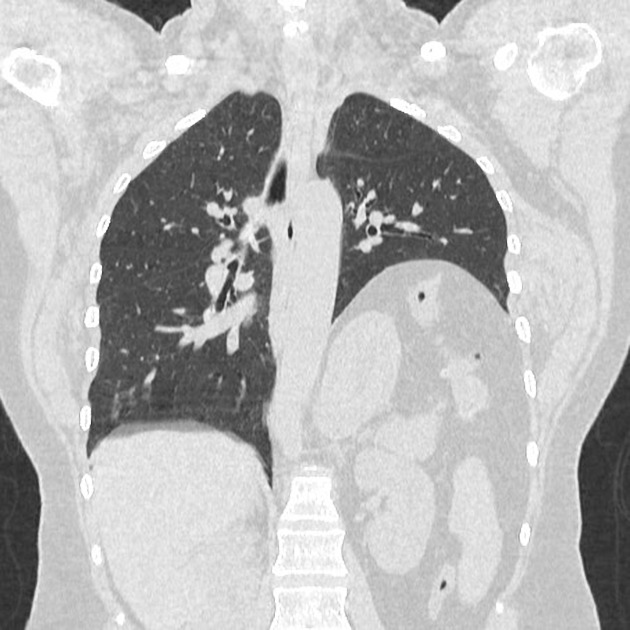
CT
On CT, atrophy of one or both diaphragmatic crura is seen and interval atrophy will be seen if there is prior imaging. The costophrenic recesses are obliterated by the flaccid diaphragm in contrast to eventration which typically affects the anterior diaphragm and has a normal posterior costophrenic recess.
Treatment and prognosis
Patients with unilateral diaphragmatic paralysis do not usually require treatment in the absence of comorbidities. In contrast, BDP may require nocturnal non-invasive positive pressure ventilation. There may be a case for phrenic nerve stimulation in some cases.
Differential diagnosis
On a chest radiograph consider:
subdiaphragmatic mass



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.