Endovascular clot retrieval (ECR)
Updates to Article Attributes
Mechanical thrombectomy for acute ischaemic stroke is the endovascular retrieval of clots obstructing large intracranial vessel in acute ischemic stroke patients.
History
In 2015, multiple randomized controlled trials showed improved clinical outcome in patients with acute stroke due to large vessel occlusion undergoing thrombectomy compared to medical treatment alone.
Indications
- Acute ischaemic stroke due to large vessel occlusion in the anterior circulation within 6 hours of symptom onset.
- As of 2017, several trials are underway determining whether selected patients groups who fall outside of the 6 hour time window might also benefit from thrombectomy.
Contraindications
Procedure
Preprocedural evaluation
Non-contrast enhanced CT is used to exclude hemorrhagehaemorrhage and CT angiography to determine large vessel occlusion. Alternatively, MRI and DSA may also demonstrate the occlusion. The role of advanced imaging such as CT perfusion to determine the infarct core and penumbra size is still uncertain.
Positioning/room set up
Equipment
- Stent retrievers
- Aspiration devices
- Balloon guiding catheter
- Microcatheters
Technique
{{youtube:http://www.youtube.com/watch?v=wY3fMI7LcCY&feature=c4-overview&list=UUU84jkgqGncjlV5YTKIFMow}}
Postprocedural care
Complications
The overall complication rate is about 15%.1 Complications include:
- Intracranial haemorrhage (intracerebral or subarachnoidal)
- Emboli to new territories
- Vessel perforation
- Arterial dissection
- Vasospasm
- Vascular access site complications
Outcomes
TechnicalThe technical outcome is graded using the mTICI score. Thrombectomy is a highly effective treatment for stroke with a number needed to treat of 2.6 for the improved functional outcome. In a meta-analysis, 46% of patients treated with mechanical thrombectomy achieved functional independence (mRS 0–2 at 90 days days) compared to 27% for best medical treatment.2
See also
-<p><strong>Mechanical thrombectomy for acute ischaemic stroke</strong> is the endovascular retrieval of clots obstructing large intracranial vessel in acute <a href="/articles/ischaemic-stroke">ischemic stroke</a> patients.</p><p> </p><h4>History</h4><p>In 2015, multiple randomized controlled trials showed improved clinical outcome in patients with acute stroke due to large vessel occlusion undergoing thrombectomy compared to medical treatment alone.</p><h4>Indications</h4><ul>- +<p><strong>Mechanical thrombectomy for acute ischaemic stroke</strong> is the endovascular retrieval of clots obstructing large intracranial vessel in acute <a href="/articles/ischaemic-stroke">ischemic stroke</a> patients.</p><h4>History</h4><p>In 2015, multiple randomized controlled trials showed improved clinical outcome in patients with acute stroke due to large vessel occlusion undergoing thrombectomy compared to medical treatment alone.</p><h4>Indications</h4><ul>
-</ul><h4>Contraindications</h4><h4>Procedure</h4><h5>Preprocedural evaluation</h5><p>Non-contrast enhanced CT is used to exclude hemorrhage and CT angiography to determine large vessel occlusion. Alternatively MRI and DSA may also demonstrate the occlusion. The role of advanced imaging such as CT perfusion to determine the infarct core and penumbra size is still uncertain.</p><h5>Positioning/room set up</h5><h5>Equipment</h5><ul>- +</ul><h4>Contraindications</h4><h4>Procedure</h4><h5>Preprocedural evaluation</h5><p>Non-contrast enhanced CT is used to exclude haemorrhage and CT angiography to determine large vessel occlusion. Alternatively, MRI and DSA may also demonstrate the occlusion. The role of advanced imaging such as CT perfusion to determine the infarct core and penumbra size is still uncertain.</p><h5>Positioning/room set up</h5><h5>Equipment</h5><ul>
-</ul><h4>Outcomes</h4><p>Technical outcome is graded using the <a href="/articles/modified-treatment-in-cerebral-ischaemia-mtici-score">mTICI score</a>. Thrombectomy is a highly effective treatment for stroke with a number needed to treat of 2.6 for improved functional outcome. In a meta-analysis, 46% of patients treated with mechanical thrombectomy achieved functional independence (<a href="/articles/modified-rankin-scale">mRS</a> 0–2 at 90 days) compared to 27% for best medical treatment.<sup>2</sup></p><h4>See also</h4>- +</ul><h4>Outcomes</h4><p>The technical outcome is graded using the <a href="/articles/modified-treatment-in-cerebral-ischaemia-mtici-score">mTICI score</a>. Thrombectomy is a highly effective treatment for stroke with a number needed to treat of 2.6 for the improved functional outcome. In a meta-analysis, 46% of patients treated with mechanical thrombectomy achieved functional independence (<a href="/articles/modified-rankin-scale">mRS</a> 0–2 at 90 days) compared to 27% for best medical treatment.<sup>2</sup></p><h4>See also</h4>
Image 1 Photo ( update )

Image 2 Annotated image ( update )

Image 3 DSA (angiography) (Internal carotid artery) ( update )
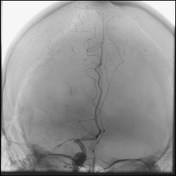
Image 4 DSA (angiography) (Common carotid artery) ( update )

Image 5 CT (C+ arterial phase) ( update )
