
Exophytic sinonasal papillomas (ESP) or fungiform sinonasal papillomas are a benign sinonasal tumour arising from the nasal septum, and one of the three main histological forms a Schneiderian papilloma can take.
On this page:
Epidemiology
Exophytic sinonasal papillomas are the second most common form of sinonasal papillomas and can occur at any age range with a peak in the third to fifth decade 1,2. They have a strong male predilection 1.
Diagnosis
The diagnosis of exophytic sinonasal papillomas is made by its septal location, endoscopic appearance and histological features 3.
Clinical presentation
Clinical symptoms are similar to the other variants and include nasal obstruction, rhinorrhoea, epistaxis and the presence of a mass lesion. They might be also found incidentally on imaging studies 3.
Pathology
Exophytic sinonasal papilloma arise from the Schneiderian epithelium of the nasal septum.
Aetiology
Low-risk human papillomavirus, in particular, type 6 and 11 are considered to have a role in their aetiology 1,2.
Location
Exophytic sinonasal papillomas are typically located anteriorly in the nasal septum 1-4. Rarely, they can arise from the middle turbinate or the nasal vestibule 3.
Subtypes
Subtypes of exophytic sinonasal papillomas include:
transitional cell papilloma
fungiform papilloma
squamous papilloma
Ringertz tumour
everted papilloma
Macroscopic appearance
Macroscopically exophytic sinonasal papillomas display the following features 1-4:
exophytic, papillary or verrucoid, cauliflower-like growth
fleshy, pink to a tannish colour
firm consistency
stalk
Microscopic appearance
Histologically primary exophytic sinonasal papillomas resemble squamous papillomas of other organs 1-4:
papillary or exophytic frond-like growth pattern around fibrovascular cores
most often well-differentiated squamous epithelium
variably transitional or columnar epithelium
hyperchromasia
some keratinisation
fewer mucocytes and intraepithelial mucous cysts
variable koilocytic changes
Radiographic features
Exophytic sinonasal papillomas usually arise from the nasal septum 5.
CT
They may appear as an isodense, unilateral mass in the nasal cavity or sinus without calcification, but cannot be readily differentiated from retained mucous or inflamed mucosa. Sometimes they may thin or destroy the adjacent bone 7.
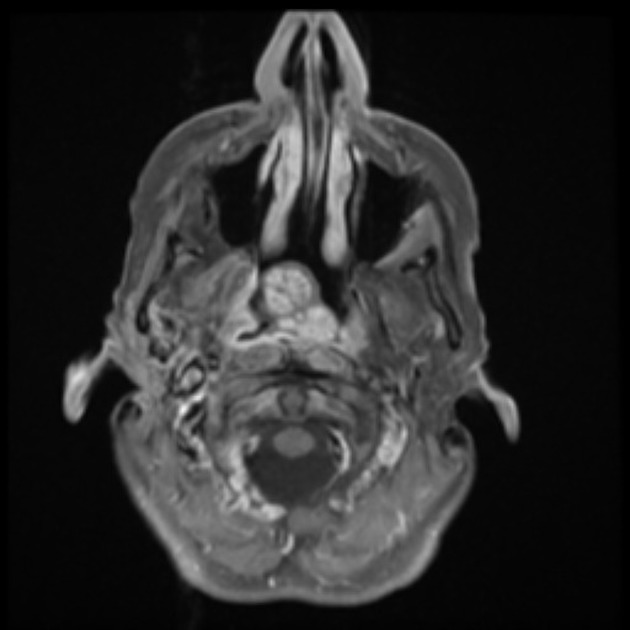
MRI
Exophytic sinonasal papillomas might show striations within the mass 3.
Signal characteristics
T1: iso to hyperintense
T2: hyperintense
T1 C+(Gd): homogeneous enhancement (less than surrounding mucosa)
Radiology report
The radiological report should include a description of the following features:
location and size of the lesion
presence of a stalk
associated focal hyperostosis
Treatment and prognosis
Treatment includes resection with clear margins. If there is no evidence of carcinoma long term prognosis is even better than with the other two variants 1,3. Recurrences can happen in cases of incomplete excisions but are less common than with the other two variants 3,4.
History and etymology
The first histological-based classification of sinonasal papillomas into inverted, cylindrical cell 'fungiform papillomas' was undertaken by VJ Hyams in 1971 1,6.
Differential diagnosis
The differential diagnosis of exophytic sinonasal papillomas include the following 6:
cutaneous squamous papilloma


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}