
Femoral artery access is a cornerstone in interventional radiology and cardiology, enabling endovascular interventions such as angiography, stent placement, and embolisation. Despite the advent of alternative access sites like the radial and brachial arteries, given reduced radiation exposure, the femoral artery remains a preferred choice for large-bore catheters and complex procedures due to its ease of access and direct route to the central vasculature 1,2.
On this page:
Indications
Femoral artery access is indicated for a wide variety of diagnostic and therapeutic procedures 3, 4:
peripheral angiography and intervention
cardiac catheterisation, especially in the absence of suitable radial access
embolisation procedures
large-bore catheter placement, e.g. intra-aortic balloon pump, Impella devices
Contraindications
local infection or groin haematoma
severe peripheral arterial disease at the access site
uncorrectable coagulopathy
previous extensive groin surgery, e.g. femoral bypass grafts
allergy to procedural materials, e.g. contrast agent
Procedure
Preprocedural evaluation
withholding anticoagulants pre-procedure if not contraindicated
patient positioned supine with the hip extended and externally rotated
sterile field and septic technique to minimise infection risk
-
anatomic localisation of the puncture site
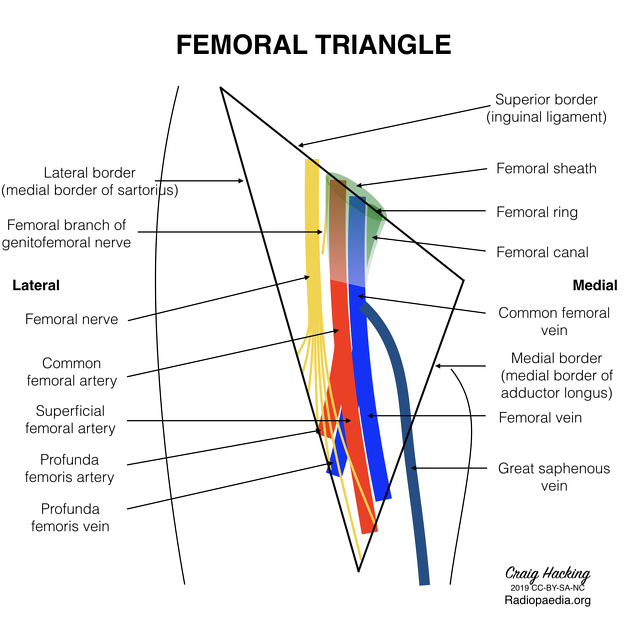
the common femoral artery (CFA) midpoint is the ideal puncture site to minimise complications related to arterial bifurcation or inguinal ligament puncture 5
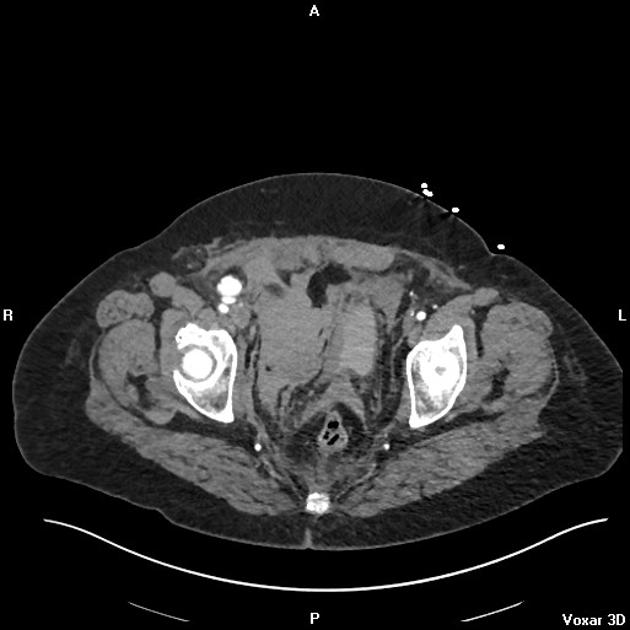
palpate the femoral pulse +/- use ultrasound guidance to visualise the CFA and its bifurcation
Technique
Three puncture techniques of femoral artery access are reported: best pulse, fluoroscopy-guided, and ultrasound directed. Compared to fluoroscopy-guided technique, ultrasound-guided femoral artery access has a higher first pass success rates, reduced mean time to access, and reduced rates of access related complications 6.
A combined ultrasound/fluoroscopy technique is as follows 3:
Local anaesthetic: Short-acting local anaesthetic is injected under real-time ultrasound visualisation.
Needle insertion: Using a 21 G or 18 G needle, puncture the CFA under real-time ultrasound guidance, ensuring the needle is inserted at a 30–45° angle.
Guidewire insertion: Advance a guidewire through into the CFA, confirming intraluminal placement using fluoroscopy.
Sheath placement: Insert the arterial sheath over the guidewire, ensuring smooth passage without resistance.
Postprocedural care
haemostasis can be achieved via manual compression, closure devices, or mechanical compression systems 4, 7-8
observe for signs of bleeding, haematoma, or pseudoaneurysm 7
standard post-procedure protocols typically involve 2–6 hours of bed rest, depending on anticoagulation use 7, 9
Complications
Femoral artery access can have complications in both the immediate and delayed settings 5, 7, 10.
Immediate complications
bleeding, haematoma
arterial dissection or occlusion
local infection
Delayed complications
chronic arterial insufficiency
Practical points
real-time ultrasound visualisation reduces complications and improves first-pass success rates
puncture site selection: avoid the CFA bifurcation and inguinal ligament to minimise complications
-
operator experience: adequate training and supervision are crucial for minimising adverse events



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.