Citation, DOI, disclosures and article data
Citation:
Weerakkody Y, Haouimi A, Shah V, et al. Fitz-Hugh-Curtis syndrome. Reference article, Radiopaedia.org (Accessed on 30 Mar 2025) https://doi.org/10.53347/rID-8227
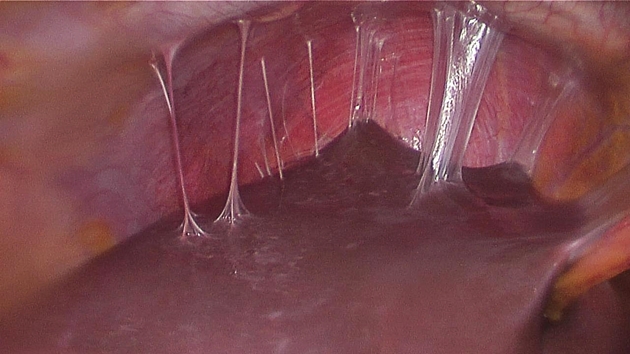
Fitz-Hugh-Curtis syndrome (FHCS), or perihepatitis, is the inflammation of the liver capsule and overlying peritoneum associated with adhesion formation, without the involvement of the hepatic parenchyma. It is a chronic complication of pelvic inflammatory disease (PID).
The prevalence in women with mild to moderate pelvic inflammatory disease may approximate 4% 10. The prevalence may be higher in genital tuberculosis 12. It most commonly occurs in women of childbearing age; however, there have been rare cases reported in males 7,8.
Patients often present with a new-onset right upper quadrant or pleuritic chest pain on a background of pelvic inflammatory disease.
It is thought to result from the direct intraperitoneal spread of infection towards the perihepatic region from initial pelvic inflammation/infection.
Diagnosis may be confirmed by the presence of Chlamydia trachomatis (most common 13) or Neisseria gonorrhea in fluid from the peritoneal cavity. Trichomonas vaginalis, Ureaplasma urealyticum and Mycoplasma hominis are less common causes of Fitz-Hugh-Curtis syndrome 9.
It has been demonstrated to occur in genital tuberculosis as well, and Mycobacterium tuberculosis may even be the dominating etiologic agent in endemic areas of developing countries 11,12.
CT
Shows inflammatory changes in both pelvic and perihepatic regions.
Pelvic findings:
Perihepatic findings:
History and etymology
The syndrome was originally described by Arthur H Curtis in 1930 and Thomas Fitz-Hugh Jr in 1934.
Imaging differential considerations include:
-
peritoneal carcinomatosis: shows more peritoneal nodularity and a solid component, overt pelvic malignancy on imaging and has a different clinical presentation
-
appendicitis: interestingly, both as differential diagnosis and possible complication 9
A 55 year old female presents to ED with right upper quadrant pain, fever and jaundice. A CT with IV contrast is performed which demonstrates a heterogeneous appearance of the liver with abnormal dilatation of the intra- and extrahepatic ducts. The gallbladder is normal with no cholelithiasis or choledocholithiasis seen. What is the most likely diagnosis?
-
1. Sam JW, Jacobs JE, Birnbaum BA. Spectrum of CT findings in acute pyogenic pelvic inflammatory disease. Radiographics. 22 (6): 1327-34. doi:10.1148/rg.226025062 - Pubmed citation
-
2. Kim S, Kim TU, Lee JW et-al. The perihepatic space: comprehensive anatomy and CT features of pathologic conditions. Radiographics. 27 (1): 129-43. doi:10.1148/rg.271065050 - Pubmed citation
-
3. Pickhardt PJ, Fleishman MJ, Fisher AJ. Fitz-Hugh-Curtis syndrome: multidetector CT findings of transient hepatic attenuation difference and gallbladder wall thickening. AJR Am J Roentgenol. 2003;180 (6): 1605-6. AJR Am J Roentgenol (full text) - Pubmed citation
-
4. Mesurolle B, Mignon F, Gagnon JH. Fitz-Hugh-Curtis syndrome caused by Chlamydia trachomatis: atypical CT findings. AJR Am J Roentgenol. 2004;182 (3): 822-4. AJR Am J Roentgenol (full text) - Pubmed citation
-
5. Cho HJ, Kim HK, Suh JH et-al. Fitz-Hugh-Curtis syndrome: CT findings of three cases. Emerg Radiol. 2008;15 (1): 43-6. doi:10.1007/s10140-007-0635-8 - Pubmed citation
-
6. Kim JY, Kim Y, Jeong WK et-al. Perihepatitis with pelvic inflammatory disease (PID) on MDCT: characteristic findings and relevance to PID. Abdom Imaging. 2009;34 (6): 737-42. doi:10.1007/s00261-008-9472-9 - Pubmed citation
-
7. Saurabh S, Unger E, Pavlides C. Fitz-hugh-curtis syndrome in a male patient: a case report and literature review. Case Rep Surg. 2012;2012: 457272. doi:10.1155/2012/457272 - Free text at pubmed - Pubmed citation
-
8. Baek HC, Bae YS, Lee KJ et-al. A case of Fitz-Hugh-Curtis syndrome in a male. Korean J Gastroenterol. 2010;55 (3): 203-7. Pubmed citation
-
9. Kazama I, Nakajima T. A case of fitz-hugh-curtis syndrome complicated by appendicitis conservatively treated with antibiotics. Clin Med Insights Case Rep. 2013;6: 35-40. doi:10.4137/CCRep.S11522 - Free text at pubmed - Pubmed citation
-
10. Risser WL, Risser JM, Benjamins LJ et-al. Incidence of Fitz-Hugh-Curtis syndrome in adolescents who have pelvic inflammatory disease. J Pediatr Adolesc Gynecol. 2007;20 (3): 179-80. doi:10.1016/j.jpag.2006.08.004 - Pubmed citation
-
11. Sharma JB, Malhotra M, Arora R. Fitz-Hugh-Curtis syndrome as a result of genital tuberculosis: a report of three cases. Acta Obstet Gynecol Scand. 2003;82 (3): 295-7. Pubmed citation
-
12. Sharma JB, Roy KK, Gupta N et-al. High prevalence of Fitz-Hugh-Curtis Syndrome in genital tuberculosis. Int J Gynaecol Obstet. 2007;99 (1): 62-3. doi:10.1016/j.ijgo.2007.03.024 - Pubmed citation
-
13. Hajira Basit, Alexander Pop, Ahmad Malik, Sandeep Sharma. Fitz-Hugh-Curtis Syndrome. (2020) Pubmed
Multiple choice questions:
Promoted articles (advertising)





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}