
Intraosseous pneumatocysts are acquired well-circumscribed gas-containing bone lesions.
On this page:
Epidemiology
These lesions are acquired and are rare in children but common in adults with an incidence around 9% 5,6.
Diagnosis
Lesions are typically identified as incidental findings on radiographs, CT scans or MRI scans.
Clinical presentation
Lesions are typically asymptomatic but can cause pain in divers due to changes in pressure and volume 9.
Pathology
The pathogenesis is uncertain. Lesions are typically associated with degeneration in the associated joint or end plate. At other sites spontaneous involution of ganglion cysts may be responsible.
Radiographic features
Location
Reported sites include 3,7,8,10:
vertebral bodies 25%
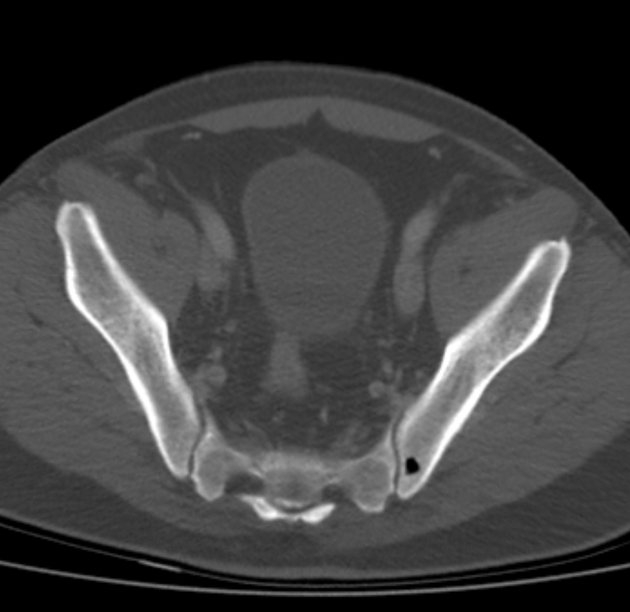
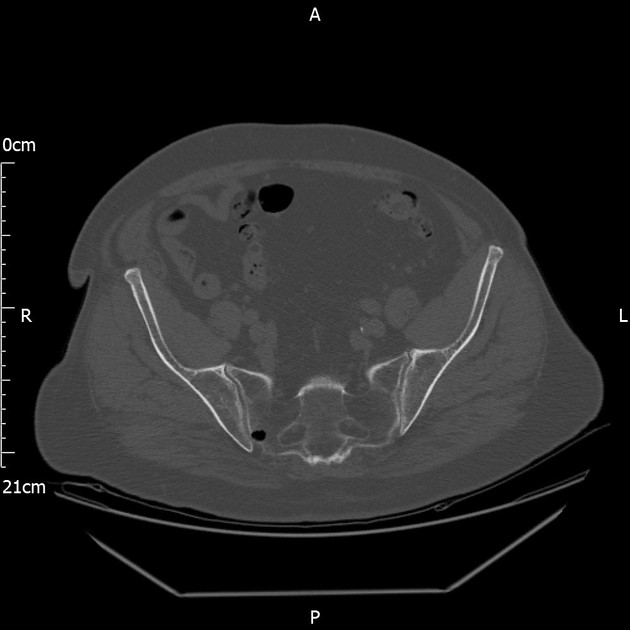
adjacent to sacroiliac joints 67%, iliac > sacral and usually male
shoulder girdle, cervical rib, pubis, posterior vertebral elements (all uncommon)
Radiography
Lytic lesions may mimic myeloma, metastasis, subchondral cyst, intraosseous lipoma or intraosseous disc herniation (Schmorl node).
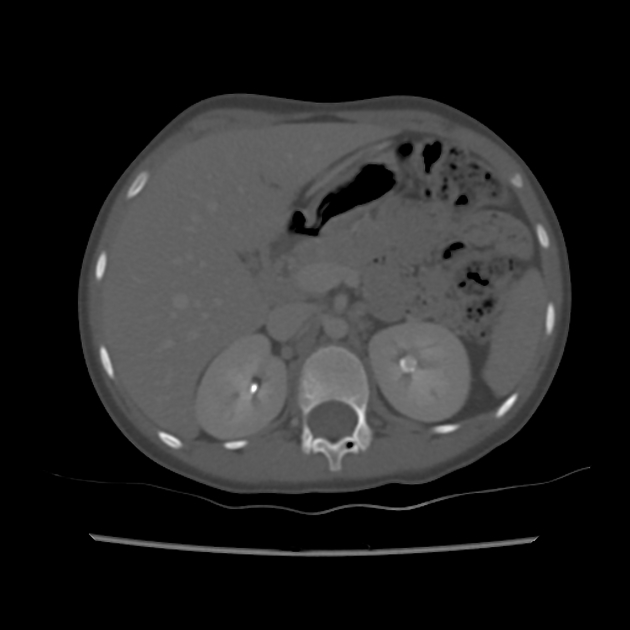
CT
CT is useful to further characterize lesions and avoid misdiagnosis on radiography or MRI. Lesions appear as well-circumscribed gas-attenuation (approximately -1000 HU) with rounded or irregular thin sclerotic margins, usually abutting a joint or vertebral end plate. Sometimes communication with an adjacent joint or end plate erosion is seen.
MRI
Signal void on both T1 and T2 weighted MR images could be mistaken for a benign or malignant sclerotic lesion. Correlation with radiography or CT can avoid misdiagnosis.
Treatment
These are don’t touch lesions; no intervention or treatment is indicated.
History and etymology
Intraosseous pneumatocysts were first reported by Ramirez in 1984 4.
Differential diagnosis
Other lesions that can cause intraosseous gas such as osteomyelitis, osteonecrosis or intraosseous disc herniations (Schmorl nodes) are readily differentiated by CT or MRI.
MRI may mimic osteoblastic lesions or kyphoplasty but these are readily differentiated by X-ray or CT.
Correct differentiation from subchondral cysts and intraosseous lipomas highlights the importance of measuring X-ray attenuation and appropriate windowing.
Practical points
Correct diagnosis relies on good radiologist technique with attention to careful analysis of CT attenuation values and use of appropriate windowing.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.