
Kaposi sarcoma (KS) is a low-to-intermediate grade mesenchymal tumour that involves the lymphovascular system. The tumour can involve the pulmonary, gastrointestinal, cutaneous and musculoskeletal systems. Although it is often thought of as an AIDS-related condition, it may also be seen in other patient groups.
On this page:
Epidemiology
Associations
lymphoproliferative disorders (particularly with the classic form)
Pathology
There are four recognised variants 1:
classic (chronic): multiple distal lower extremity predominant purple skin plaques and rarely involve visceral organs
endemic (lymphadenopathic): common in equatorial Africa
iatrogenic (organ transplant-related)
AIDS-related (epidemic): usually requires the CD4 count to drop <200 cells/mm3; may develop in up to 35% of patients with AIDS 2 and when developed it is considered an AIDS-defining illness
The latter two variants are much more common.
Aetiology
Kaposi sarcoma is caused by infection with human herpesvirus-8 (HHV-8), also known as Kaposi sarcoma-associated herpesvirus (KSHV) 9. The AIDS-related and post-transplant variants are also associated with immunosuppressive states.
Microscopic appearance
Histologically can comprise of sheets of plump spindle-shaped cells surrounding and lining slit-like vascular spaces.
Radiographic features
There is a wide spectrum of imaging findings depending on which organ is involved. However, most features are non-specific 1,2,4 but may assist in diagnosis if relevant clinical risk factors (e.g. background AIDS history) are evident. In 30% of cases, there is no concurrent cutaneous involvement 1.
Plain radiograph
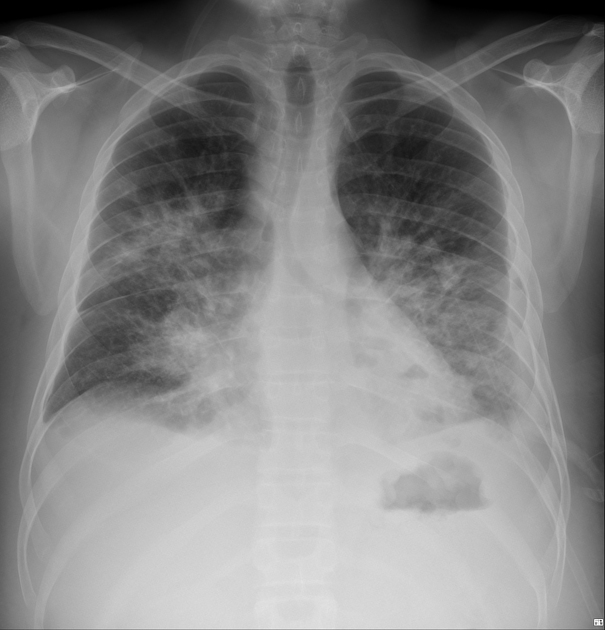
The following features may be seen on chest radiographs:
-
parenchymal nodular or reticular opacities with a predilection towards perihilar mid to lower zones; has two major patterns
linear interstitial nodules
fluffy ill-defined nodules
mediastinal and/or hilar lymphadenopathy
CT
On HRCT of the chest:
-
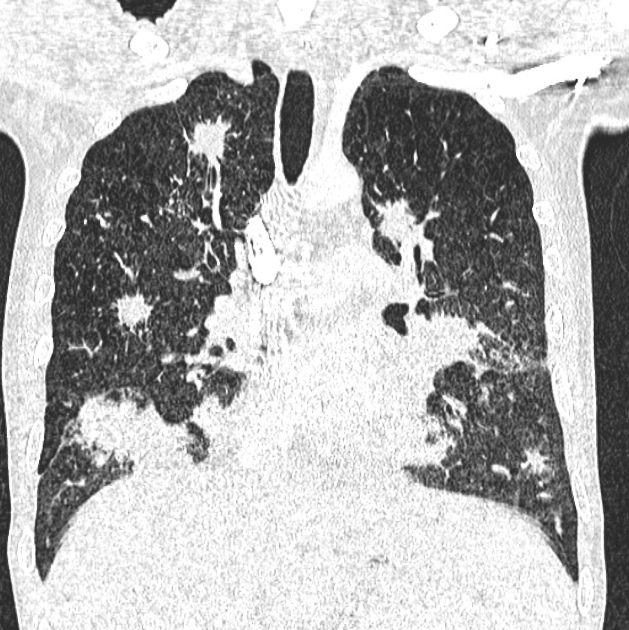
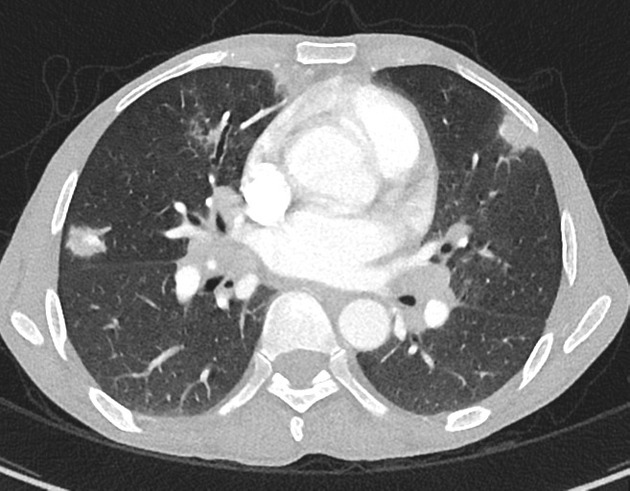
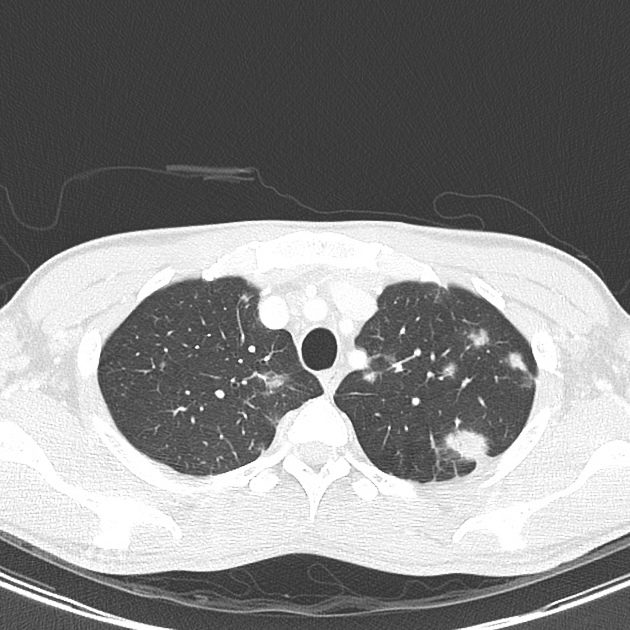
ill-defined (flame-shaped) nodular opacities with usually bilateral and roughly symmetrical perilymphatic and peribronchovascular distribution (typically >1 cm in diameter) 1
may have surrounding patchy ground glass changes
-
lymphadenopathy (may be present in up to 50%) 5
typically of high attenuation 6
-
less commonly it may present as asymmetrically distributed nodules or
larger masses1
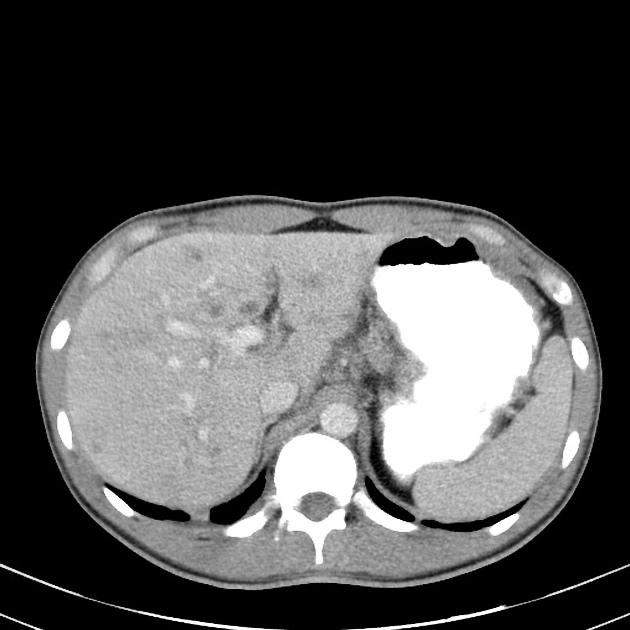
On liver CT:
ill-defined multifocal peripheral portal nodules with variable attenuation (commonest hepatic neoplasm in AIDS patients) 1,4
Nuclear medicine
Scintigraphy may be useful if concurrent opportunistic infection or lymphoma is suspected:
thallium-201: usually positive in both lymphoma and Kaposi sarcoma
gallium-67: usually negative in Kaposi sarcoma but positive in lymphoma and infection
History and etymology
This condition was first described by Moritz Kaposi (1837-1902), an Austro-Hungarian dermatologist, in 1872.
Differential diagnosis
For thoracic involvement consider:
lymphoma (AIDS-related lymphoma: ARL): appear more well defined
fungal (e.g. angioinvasive aspergillosis) or mycobacterial infection
bacillary angiomatosis: also has skeletal lesions





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}