
Laryngomalacia is the most common cause of noisy breathing in infants where it results in stridor. It is the result of a congenital abnormality of the cartilage in the larynx that results in the dynamic partial supraglottic collapse of the larynx during breathing.
On this page:
Clinical presentation
Most children present in early infancy with stridor. Symptoms are maximal around 6-8 months and the symptoms will have resolved in most by 12-24 months.
It may be associated with feeding difficulties in some patients and it is frequently seen in combination with gastro-esophageal reflux disease.
Laryngomalacia can also occasionally present in adults 3.
Pathology
Laryngeal collapse occurs in the inspiratory phase of breathing when an anatomical abnormality results in intermittent upper airway obstruction and stridor.
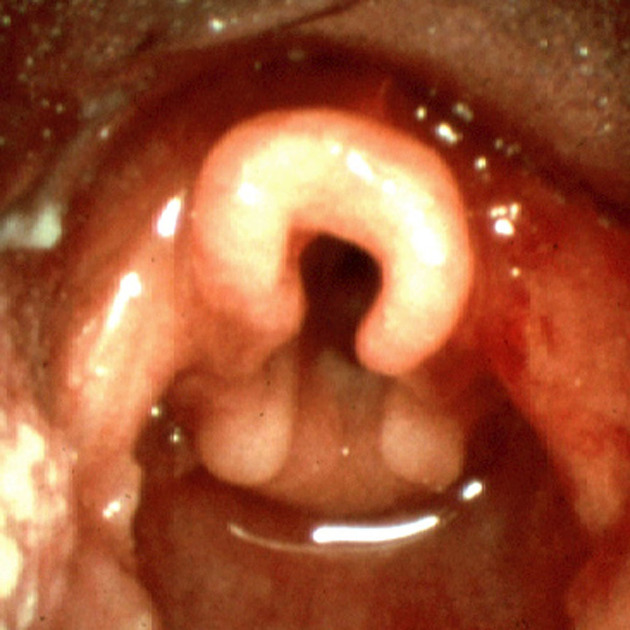
The underlying anatomical abnormality is most commonly shortening of the aryepiglottic folds (see types below), resulting in side-to-side curling of the epiglottis. However, prolapse of supraglottic tissues into the laryngeal inlet during inspiration may also be the cause. The epiglottis, aryepiglottic folds and corniculate mounds of the arytenoids may be involved 1.
Some authors suggest that mucosal inflammation as the result of gastro-esophageal reflux disease (GERD) may also be an etiological consideration 2. Where there is suspicion of GERD, it should be treated.
Types
The most commonly used classification, proposed by Olney et al. classifies to 3 types as follows 4
type 1: prolapse of the mucosa overlying the arytenoid cartilages
type 2: foreshortened aryepiglottic folds
type 3: posterior displacement of the epiglottis
Radiographic features
The diagnostic investigation of choice is flexible laryngoscopy. Radiology is often not involved.
Patients may have chest radiographs because of associated chest findings, or upper-GI contrast studies to assess gastro-esophageal reflux disease. They may also have chest cross-sectional imaging or ultrasound to make an assessment of the subglottic space and exclude a subglottic lesion.
Treatment and prognosis
Treatment is largely supportive since most children show spontaneous resolution after 12-24 months. When associated gastro-esophageal reflux disease is present, that should be treated. Endoscopic supraglottoplasty may be required in severe cases where there is significant airway obstruction.
Differential diagnosis
congenital tracheal anomalies, e.g. tracheomalacia


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.