
The lesser sac or omental bursa is a potential peritoneal space within the abdomen, part of the peritoneal cavity.
On this page:
Gross anatomy
The lesser sac may be conceptualized as the space posterior to the lesser omentum, between the posterior wall of the stomach and the surface of the peritoneum that covers the anterior surface of the left kidney 1.
The epiploic foramen (of Winslow) is the only natural communication between greater and lesser sacs 3.
Boundaries
As the lesser sac is a peritoneal space, all of its boundaries are lined by visceral or parietal peritoneum 3. On the left side, the lesser sac is partially divided by a peritoneal fold over the left gastric fold, named pancreatogastric fold 3.
-
anterior
lesser omentum
visceral peritoneum along the posterior surface of the stomach
gastrocolic omentum (between greater curvature of the stomach and transverse colon)
-
left lateral
gastrosplenic and splenorenal ligaments
-
right lateral
epiploic foramen (of Winslow) communicating with greater sac
-
posterior
visceral/parietal peritoneum that covers the diaphragm, pancreas, left kidney/adrenal gland, and duodenum
transverse mesocolon (between the transverse colon and anterior surface of the pancreas)
-
superior
peritoneum covering the caudate lobe of the liver
Recesses
superior (hepatic) recess - between caudate lobe of liver and diaphragm; it is partially separated from splenic recess by gastropancreatic fold
splenic recess - between splenic ligaments and stomach
inferior (omental) recess - between the stomach and transverse colon
Radiographic features
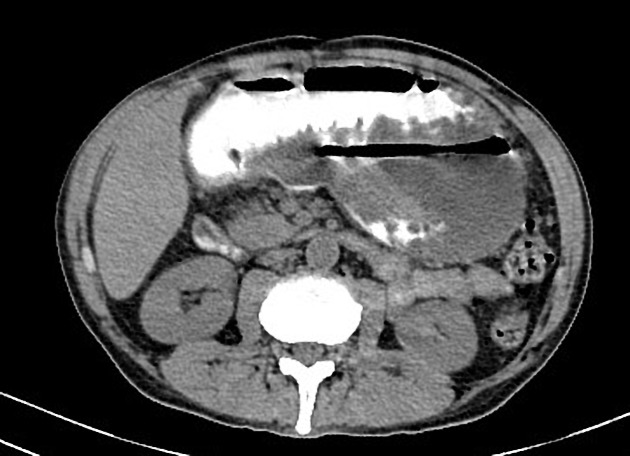
CT
In healthy patients the lesser sac is typically collapsed 4. A large amount of fluid within the lesser sac is usually due to an inflammatory process of the adjacent organs (stomach, pancreas, or duodenum) and thus is always exudative in nature 4.
In patients with generalised oedema and ascites (e.g. renal and liver failure), the volume of transudative fluid in the greater sac is much larger than the lesser sac 4.
Masses within lesser sac may be neoplastic or non-neoplastic. Primary tumours of the lesser sac are rare with metastases being more common 4. Primary malignant neoplastic masses of the lesser sac include liposarcoma, leiomyosarcoma, and malignant gastrointestinal stromal tumours 4. Benign tumours of the lesser sac include lymphangiomas and teratomas 4.
Development
The lesser omentum is composed of two peritoneal ligaments that extend from the lesser curvature of the stomach and duodenal bulb to the liver, the gastrohepatic, and hepatoduodenal ligaments, respectively. During embryologic development, the rotation of the stomach relative to the liver causes redundancy in the mesentery about the stomach.
As the greater curvature of the stomach rotates anterolaterally, a recess is formed between the redundant dorsal peritoneal ligament connecting the greater curvature of the stomach to the dorsal abdominal wall. Simultaneously, the lesser curvature of the stomach rotates posteromedially, and the ventral peritoneal ligament between stomach and liver becomes the lesser omentum, an incomplete boundary separating the main peritoneal cavity (greater sac) from the posterior recess (lesser sac).




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}