
Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) represents a group of inflammatory demyelinating disorders united by the presence of IgG antibodies to myelin oligodendrocyte glycoprotein (MOG). MOGAD represents a distinct clinical entity that clinically overlaps but is nonetheless separate from acute disseminated encephalomyelitis (ADEM), neuromyelitis optica spectrum disorder (NMOSD) and multiple sclerosis (MS).
On this page:
Terminology
As research was undergoing into MOGAD, many alternate terms were used in the literature, including MOG-IgG-associated optic neuritis, encephalitis, and myelitis (MONEM), anti-MOG associated encephalomyelitis, anti-MOG encephalitis and other variations on this theme 1-4.
Epidemiology
MOGAD is primarily encountered in children and young adults 1 with an estimated incidence of between 1.6 and 3.4 per 1,000,000 person-years 13 and a median age onset between 20-30 years. No sex difference in prevalence have been described 14. In children with acquired demyelination syndrome, MOG-IgG is more commonly detected than aquaporin-4 antibodies 5.
Additionally, children with MOGAD are more likely to present with an ADEM-like clinical picture, whereas adults are more likely to present with an NMOSD-like syndrome 5.
Clinical presentation
Clinical presentation is similar to that of other acquired demyelinating conditions and varies from individual to individual. In approximately half of cases there is viral prodrome 2.
Not all presentations are equally prevalent:
-
optic neuritis (most common, 41-63%)
this may encompass cases previously termed chronic relapsing inflammatory optic neuropathy (CRION)
-
transverse myelitis (30%) including conus medullaris syndrome
associated with longitudinally extensive spinal cord lesions
ADEM-like encephalomyelitis (2-6%)
-
cortical encephalitis with seizures
-
infratentorial syndromes (i.e. brainstem or cerebellar syndromes)
this may include a CLIPPERS-like presentation 9,10
No specific presentation distinguishes individuals with anti-MOG antibodies from those presenting with similar clinical manifestation but without the antibodies and at the time of writing (c. 2022) no single set of diagnostic criteria are universally accepted 5.
Pathology
Myelin oligodendrocyte glycoprotein (MOG) is expressed on oligodendrocytes and the outer lamellae of myelin sheaths 6.
Radiographic features
MRI
Imaging presentation of MOGAD is variable and with no pathognomonic imaging features, with patients having an imaging phenotype often indistinguishable from other inflammatory white matter diseases of the central nervous system (e.g. acute disseminated encephalomyelitis (ADEM), neuromyelitis optica spectrum disorder (NMOSD) and to a lesser degree multiple sclerosis). Nonetheless, certain imaging features are increasingly recognized as being more typical of MOGAD, allowing the diagnosis to be suspected on the basis of imaging.
Cerebral involvement
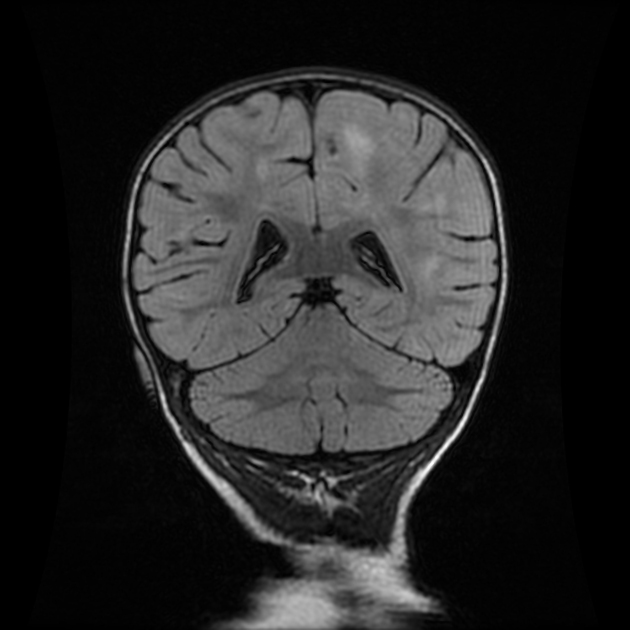
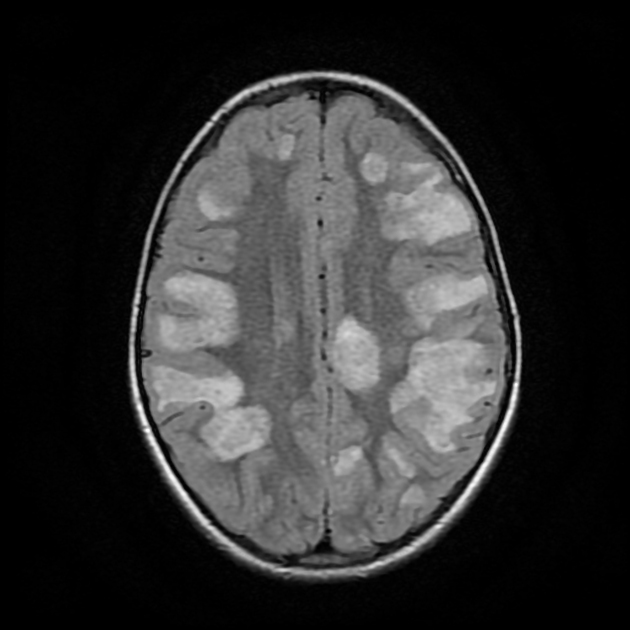
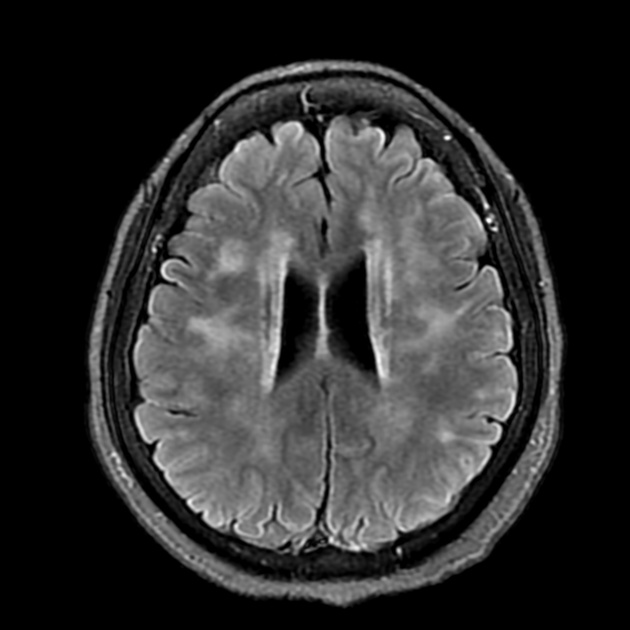
The pattern of cerebral involvement, if present, is highly variable. Acute disseminated encephalomyelitis (ADEM) is a common presenting clinical and imaging phenotype of patients with MOGAD, particularly in childhood 6. In contrast, less than half of adults presenting with MOGAD have brain lesions at the time of diagnosis.
When present, lesions tend to be few in number but sizable, typically bilateral with ill-defined borders. Deep grey matter and brainstem involvement is more common in children 6. Leptomeningeal enhancement is uncommon but encountered either in isolation or along with cortical lesions (e.g. as part of FLAMES) 6,7. Parenchymal enhancement is also variable, with brainstem, grey matter, white matter, periventricular involvement reported 11.
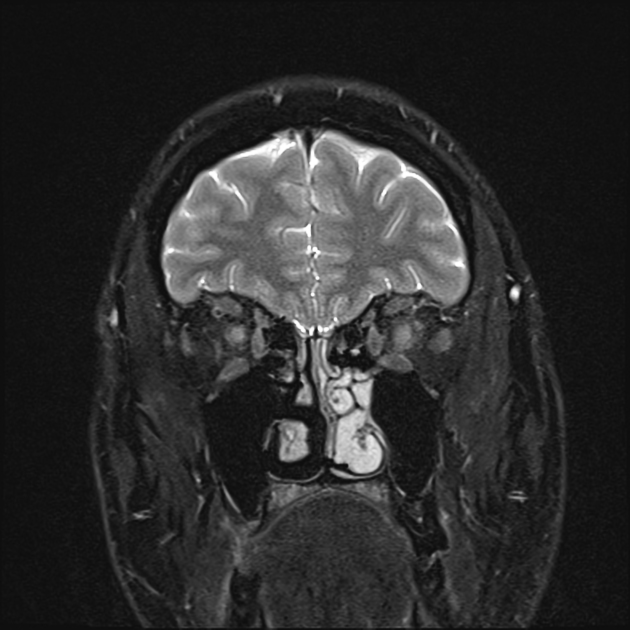
Optic nerve involvement
The optic nerves are involved in the majority of patients with MOGAD at the time of presentation (>80%) typically with bilateral optic neuritis, involving the anterior parts, with prominently swollen edematous nerves resulting in tortuosity and optic disc swelling 6. Optic perineuritis, inflammation of the optic nerve sheath, is another characteristic finding 12. There may be periorbital and intraorbital enhancement as well 8,12. Involvement of the optic chiasm and optic tracts is uncommon 6.
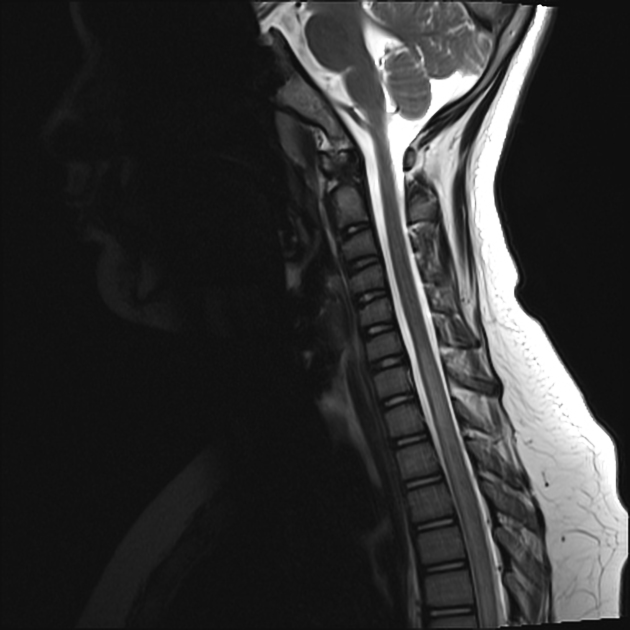
Spinal cord involvement
Spinal involvement usually is central affecting both grey matter and central white matter and can be both lengthy (longitudinally extensive spinal cord lesions) or short segment, and both patterns may be encountered simultaneously 6. The involvement of grey matter forms the H sign on axial view and thin linear T2 hyperintense signals on sagittal view 8. The lower cord is often preferentially affected, with the conus medullaris being classically affected 6. A helpful distinguishing feature is the presence of leptomeningeal enhancement, relatively common in MOGAD but rarely seen in multiple sclerosis and NMOSD 6.
Treatment and prognosis
Although treatment and prognosis remain to be fully understood, it appears that generally, individuals with anti-MOG antibodies have fewer relapses and less severe clinical course than individuals with anti-aquaporin 4 antibodies presenting with NMOSD 2.
Acute management with intravenous methylprednisolone, plasma exchange, intravenous immunoglobulin or cyclophosphamide have been reported and appear to be efficacious 2.
It remains unclear what, if any, long-term medications are required in individuals with a relapsing time course, although it seems that response to immunotherapeutic agents is different to multiple sclerosis and that some agents efficacious in the latter may actually worsen anti-MOG related diseases 2.
Differential diagnosis
-
neuromyelitis optica spectrum disorder (NMOSD): although in many ways similar, a number of features are helpful in distinguishing individuals with aquaporin-4-IgG-positive NMOSD from those with MOGAD
optic neuritis in patients with MOGAD typically primarily affects only the anterior optic nerves and optic nerve sheaths (optic perineuritis), which are severely swollen, edematous and tortuous, generally sparing the optic chiasm and tracts 6
brain lesions in MOGAD are more commonly seen involving the thalami, pons, whereas involvement of the area postrema and medulla is uncommon 6
-
multiple sclerosis: generally, the typical features encountered in multiple sclerosis are absent in MOGAD
Dawson fingers are absent in MOGAD
spinal involvement in MOGAD is often longitudinally extensive rather than short
brain lesions in MOGAD, when present, are larger and fewer in number in an ADEM-like pattern 6
optic neuritis in MOGAD is usually bilateral and more longitudinally extensive 6 and more commonly involves the anterior portion of the optic nerves 15
leptomeningeal enhancement is rare in multiple sclerosis, and even if present is usually very subtle 6
acute disseminated encephalomyelitis (ADEM): can be indistinguishable both clinically and on imaging



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.