
Nephrotic syndrome results from loss of plasma proteins in the urine and characterised by hypoalbuminaemia, hyperalbuminuria, hyperlipidaemia, and oedema. It may be caused by primary (idiopathic) renal disease or by a variety of secondary causes.
On this page:
Clinical presentation
Patients present with marked oedema, proteinuria, hypoalbuminaemia, and often hyperlipidaemia 1.
Complications
Pathology
It may be classified as congenital or acquired 1:
-
congenital
-
acquired
-
primary
-
secondary
drugs, e.g. NSAIDs
infections
when no cause is identified the term adult idiopathic nephrotic syndrome is used
-
Radiographic features
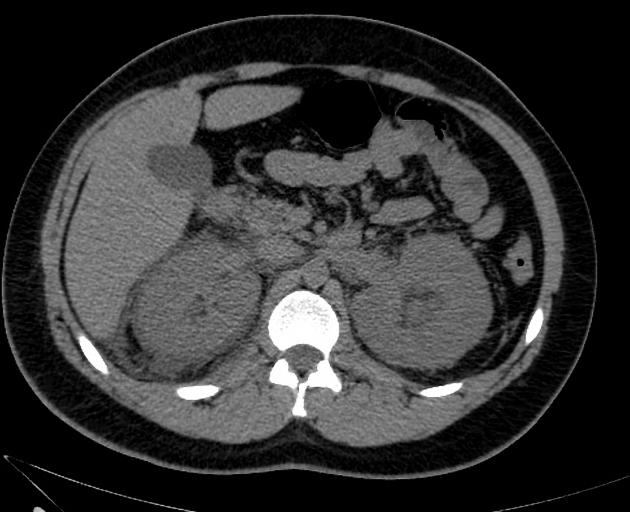
Nephrotic syndrome per se may produce non-specific appearances due to marked oedema and hypoalbuminaemia, e.g. anasarca, bowel wall thickening, etc. Chyluria may be seen due to the heavy losses of chyle/fats in the urine.
Treatment and prognosis
Treatment of most patients should include fluid and sodium restriction, oral or intravenous diuretics, and angiotensin-converting enzyme inhibitors 1,4-6. Some adults with nephrotic syndrome may benefit from corticosteroid treatment, ciclosporin A, although research data are limited 1,4-6. Intravenous albumin, prophylactic antibiotics, and prophylactic anticoagulation are not recommended 1,4-6.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.