
Odontoid process fixation or odontoid process repair refers to the surgical fixation of an odontoid fracture.
Anterior odontoid screw fixation is performed with single and double screw techniques, non-cannulated and cannulated screws, and uni- or bicortical fixation techniques.
Odontoid plate fixation has been proposed as an alternative for certain fracture patterns 2.
On this page:
History and etymology
The first anterior odontoid screw fixation was first applied by the Austrian surgeon Friedrich Paul Magerl 1978 and the Japanese surgeon T Nakanishi 3,4. Odontoid plate fixation has been first described by the Austrian surgeon R Streli in 1981 5.
Indications
Odontoid process fixation is typically performed in the clinical setting of odontoid fractures:
- Anderson d’Alonzo type II (ideally with an anterosuperior to posteroinferior course)
- Anderson d’Alonzo type III (high/shallow type)
Contraindications
Contraindications of anterior odontoid screw or plate fixation include the following:
- intraarticular atlantoaxial joint injuries
- Jefferson fracture
- transverse alar ligament injury/disruption
- pathological odontoid fracture
A further contraindication to anterior odontoid screw fixation is an oblique fracture line from posterosuperior to anteroinferior, parallel to the screw trajectory.
Procedure
The procedure and technique of odontoid screw fixation involve an anterior approach. A rough overview of the surgical procedure concerning the different techniques includes the following 1:
- anteromedial approach with exposure of the C2 body
- odontoid screw fixation
- screw entry point determination in the inferior part of the C2 endplate
- double conventional screw insertion
- screw trajectory slight posteriorly and medially angulated with the exit in the posterior half of the odontoid tip
- drilling under tissue protection and screw insertion
- double cannulated screw insertion
- K-wire placement and cortex preparation
- cannulated screw insertion under fluoroscopic guidance
- single cannulated screw insertion (young patients with good bone stock)
- slight posteriorly angulated midline screw trajectory
- K-wire placement and cortex preparation
- cannulated screw insertion under fluoroscopic guidance
- odontoid plate fixation
Complications
Complications of odontoid process fixation include the following 1,3,6:
- fracture nonunion
- persistent atlantoaxial instability
- postoperative radiculopathy (C2 nerve root pain)
- neck stiffness
-
hardware malpositioning
- spinal cord injury
- nerve root injury
- implant loosening/proximal screw back out
-
hardware failure
- proximal screw break out through the anterior C2 vertebral body
- screw bending or fracture
- pharyngeal or oesophageal perforation
- retropharyngeal haemorrhage
- airway obstruction
- aspiration/pneumonia
- dysphagia
Radiographic features
Plain radiograph
Plain radiographs can show the position of implants and evaluate bony fusion 1.
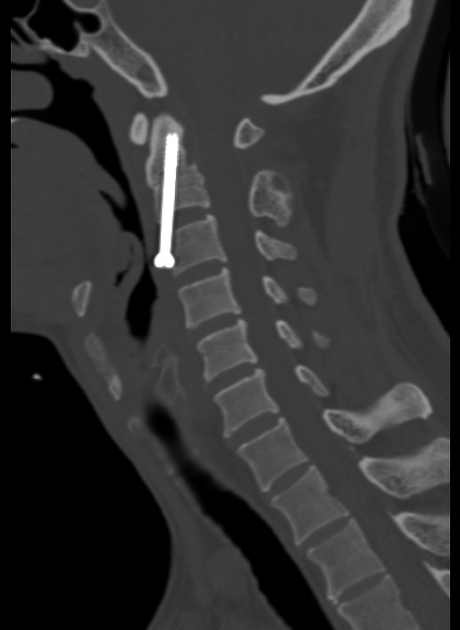
CT
In addition to the exact position of implants, CT might detect complications and characterise fracture healing.
MRI
MRI can be used to evaluate the spinal canal and the transverse alar ligament or in the setting of suspected complications 1.
Radiology report
The postoperative radiological report should include a description of the following features:
- implanted hardware
- position of screws especially with relation to the following structures
- spinal canal
- foramen transversarium
- complications
Outcomes
Anterior screw fixation of odontoid fractures features a higher bony fusion rate (>80%) as compared to non-operative management with cervical hard collar or halo vest 1. As opposed to atlantoaxial fusion techniques odontoid process fixation techniques preserve atlantoaxial motion 1,3,6.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.