
Phosphaturic mesenchymal tumours are the cause of the vast majority of cases of tumour-induced (oncogenic) osteomalacia due to the production of fibroblast growth factor-23 (FGF-23).
On this page:
Epidemiology
These tumours are extremely rare, with fewer than 500 cases reported in the literature 1. Most occur in middle-aged adults, but cases in all ages have been reported 1,2.
Clinical presentation
Patients usually present with symptoms related to hypophosphataemia, such as chronic muscle aches and weakness, and to osteomalacia, such as bone pain and multiple fractures 1. The biochemical features are hypophosphataemia, phosphaturia, and inappropriately normal or low levels of 1,25-hydroxyvitamin D (calcitriol).
Pathology
Phosphaturic mesenchymal tumours are benign spindle cell neoplasms.
Location
Phosphaturic mesenchymal tumours usually originate in a bone or soft tissue site 2.
Classification
These are tumours of uncertain differentiation in the WHO classification of soft tissue tumours.
The most common morphologic subtype is the mixed connective tissue type, which accounts for more than 70% 2. The other patterns are osteoblastoma-like, nonossifying fibroma-like, and ossifying fibroma-like.
Radiographic features
CT
The tumours are round/oval, circumscribed soft tissue masses with contrast enhancement 2. Fat or calcification may be present 1.
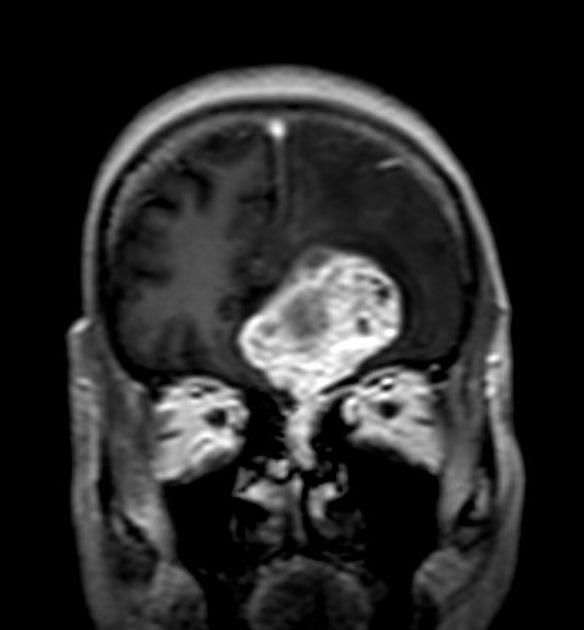
MRI
The tumours show the following signal characteristics 2:
- T2: markedly hyperintense
- T1 C-: isointense to muscle unless there is intratumoural fat or cystic change 5
- T1 C+: marked homogeneous enhancement
Larger tumours tend to be more heterogeneous in signal intensity. Vascular flow voids may be seen.
Nuclear medicine
Somatostatin receptor imaging such as gallium-68 DOTATATE and DOTANOC PET have been suggested as first-line whole-body imaging to localise a suspected tumour causing oncogenic osteomalacia 3,4.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.