
Pulmonary manifestations are relatively common in rheumatoid arthritis, and like many of its non-articular manifestations, tend to develop later in the disease.
Please refer to the related articles for a general discussion of rheumatoid arthritis, and for the specific discussion of its musculoskeletal manifestations.
On this page:
Epidemiology
Although rheumatoid arthritis is more common in women, respiratory disease more commonly develops in men 6.
Clinical presentation
Respiratory symptoms are often absent, or non-specific such as dyspnoea and chronic cough.
Pathology
Associations
bronchocentric granulomatosis: rare 7
Radiographic features
Patterns of lung involvement include interstitial, airway and pleural disease.
Pleural involvement is a common manifestation of rheumatoid arthritis, although usually asymptomatic.
pleural thickening: is seen more commonly than pleural effusions
pleural effusions: occur late in the disease, are often unilateral and associated with pericarditis and subcutaneous nodules 5
Other manifestations include:
Plain radiograph
Chest radiograph may show:
pleural effusion
lower zone predominant reticular or reticulonodular pattern
volume loss in advanced disease
skeletal changes, e.g. erosion of clavicles, glenohumeral erosive arthropathy, superior rib notching
CT
Chest CT or HRCT features include:
pleural thickening or effusion
-
interstitial fibrosis (rheumatoid arthritis associated interstitial lung disease)
-
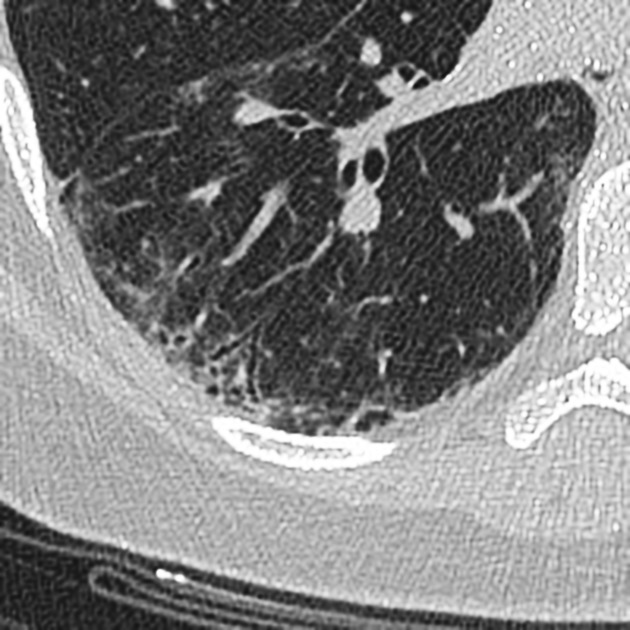
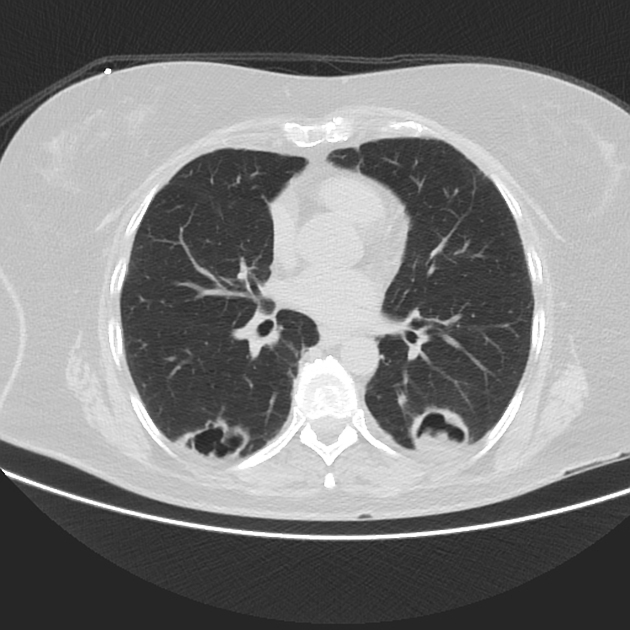
large rheumatoid nodules
single or multiple
tend to be based peripherally
may cavitate (necrobiotic lung nodules)
cavitation of a peripheral nodule can lead to pneumothorax or haemopneumothorax
-
follicular bronchiolitis: rare
small centrilobular nodules or tree-in-bud
thin-walled cysts similar to those seen in lymphocytic interstitial pneumonia can uncommonly occur 13,14




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.