
Rhombencephalitis (plural: rhombencephalitides) refers to inflammatory diseases affecting the hindbrain (brainstem and cerebellum) and has a wide variety of aetiologies including infection, autoimmune disease, and paraneoplastic syndrome, with Listeria monocytogenes being the most common cause. Rhombencephalitis carries significant morbidity and mortality.
For a specific discussion, please refer to articles:
On this page:
Terminology
It is important to remember that both terms "rhombencephalitis" and "brainstem encephalitis”, despite being used as interchangeable terms, are anatomically different, as the former includes the cerebellum as well as the brainstem.
Clinical presentation
Symptoms can vary due to the different causes of rhombencephalitis. When caused by a virus it usually presents with headache, vomiting, fever, and ill-defined neurological symptoms (the prodromal stage lasting for one to two weeks). Subsequently, patients develop a spectrum of brainstem symptomatology such as cranial nerve palsies (occur in ~75% of all cases), and cerebellar and long-tract motor and sensory deficits.
Pathology
-
infectious
-
viral
enterovirus 71: is probably the second most common of infectious rhombencephalitis
-
herpes simplex virus (HSV): is the third most common
80% are caused by HSV1
20% are caused by HSV2
human herpesvirus 6 (HHV6)
flaviviruses (e.g. West Nile virus and Japanese encephalitis virus)
JC virus (i.e. progressive multifocal leukoencephalopathy)
-
bacterial
Listeria monocytogenes: the most common cause of infectious rhombencephalitis 7
Mycobacterium tuberculosis
Rickettsia, Borrelia burgdoferi, Salmonella typhi, Legionella bozemanii and Mycoplasma pneumoniae are agents that rarely cause encephalitis, but can involve the brainstem.
-
-
autoimmune 7
Behçet disease (most common autoimmune cause)
paraneoplastic syndromes: associated with antibodies (e.g. anti-Yo, anti-Hu) and, in the majority of cases, having small cell lung cancer as the underlying cause 7
-
malignancy
lymphoma (rare)
Radiographic features
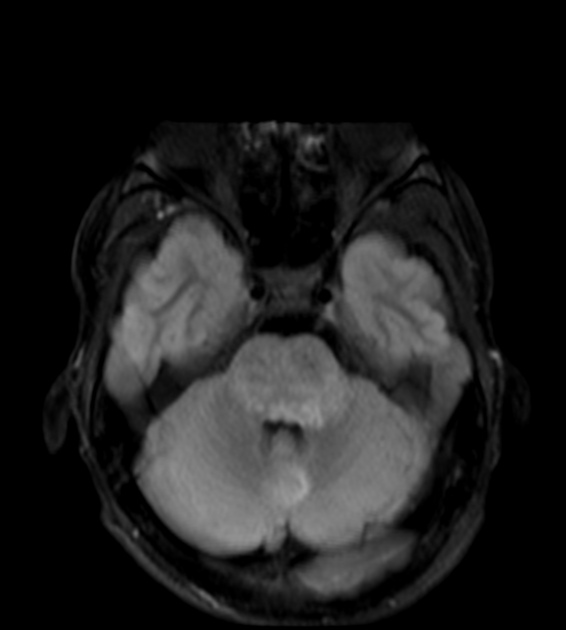
Beam-hardening artifacts limit the visualisation of the brainstem on CT images. MRI with contrast is the imaging modality of choice for the assessment of patients with suspected pathology in that anatomic location.
MRI
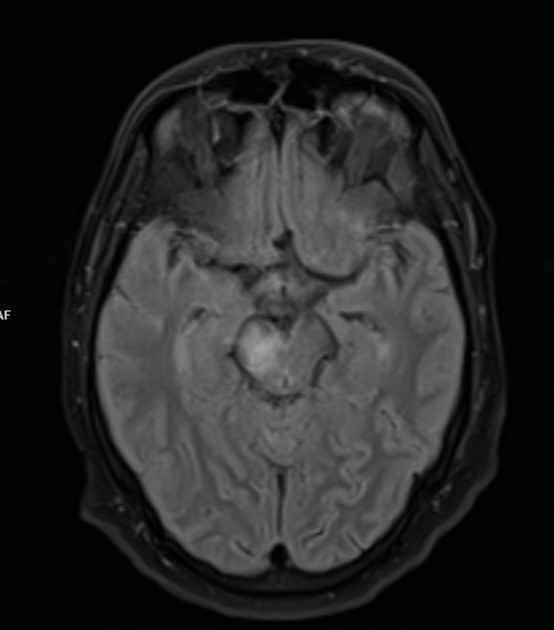
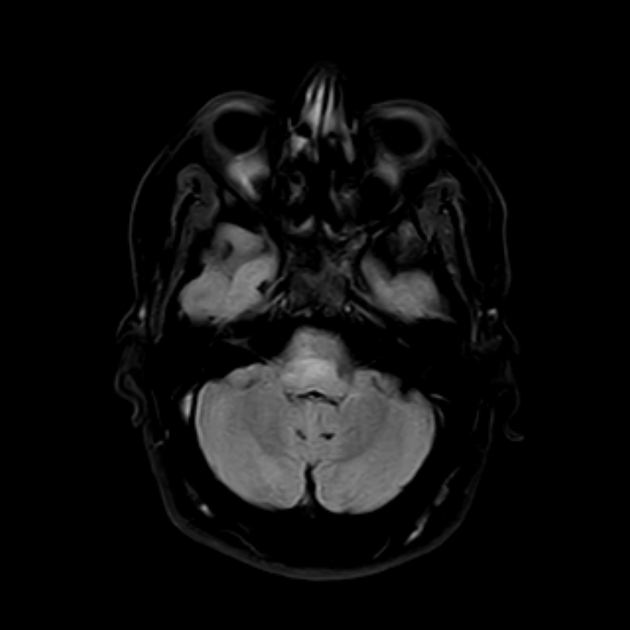
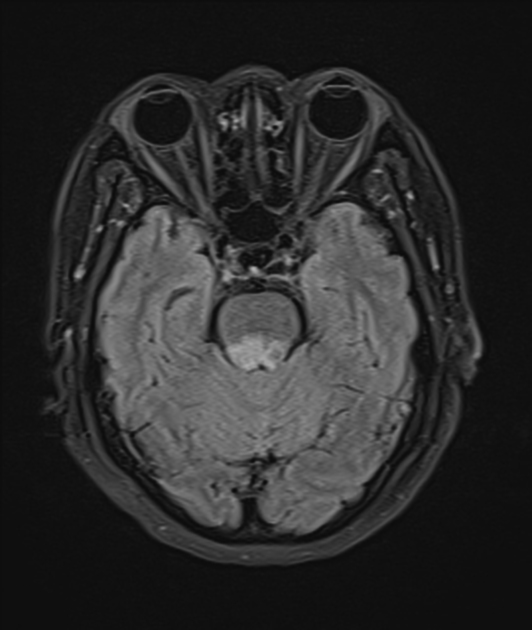
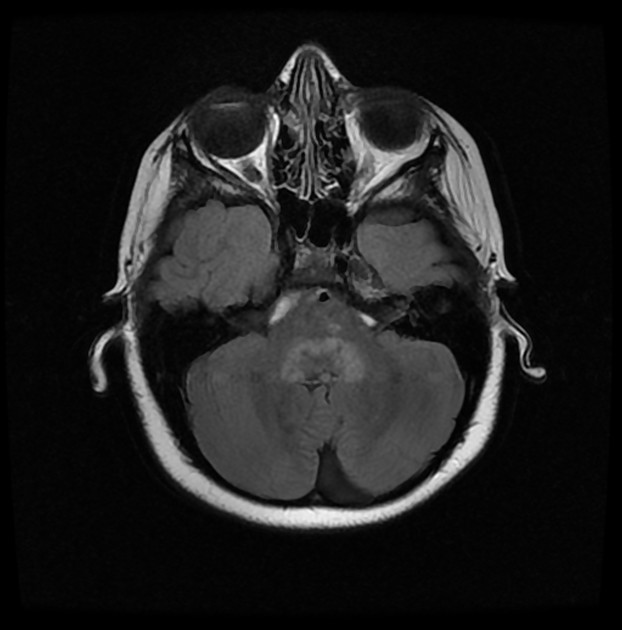
When caused by infectious agents, rhombencephalitis usually has the following signal characteristics:
T1: hypo- or isointense lesion
T2/FLAIR: hyperintense
DWI: hyperintense
ADC: hypointense
-
T1 C+ (Gd):
linear cranial nerve enhancement
ring enhancement (abscess)
heterogeneous if extensive inflammation
MR spectroscopy: allows differentiation between abscess from tumour
Treatment and prognosis
Rhombencephalitis requires early diagnosis and treatment to avoid neurological sequelae. The mortality rate is reported between 10-15% 3.
History and etymology
It was first reported by Edwin Bickerstaff and Philip Cloake in 1951 2. The term is derived from the Greek: "rhombos" (lozenge-shaped figure) and "enkephalos" (brain).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}