
A right hemicolectomy is a surgical procedure to remove the caecum and ascending colon.
On this page:
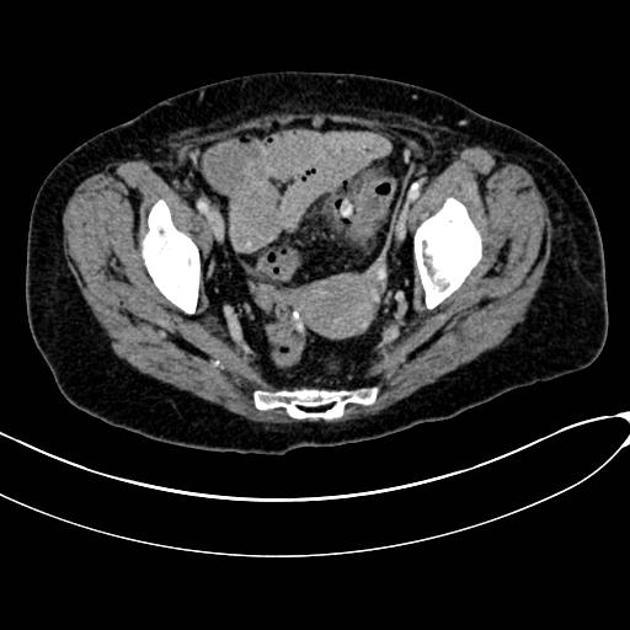
Images:
Indications
cancer of the appendix, caecum or ascending colon (most common) 1
inflammatory bowel disease, particularly Crohn's disease
complicated appendicitis
perforation of the right colon
right-sided ischaemic colitis
Procedure
Though historically an open procedure, the majority are performed laparoscopically in the elective setting, though an open procedure may be required in an emergency or case of complication. The right colon is mobilised, and the bowel is divided at the terminal ileum and typically the proximal transverse colon. To achieve a good oncological resection the associated lymphatic drainage of the tumour must also be resected, so the right colic and ileocolic arteries are divided close to their origin from the superior mesenteric artery 1. An anastomosis is formed between the terminal ileum and the remaining transverse colon. A covering loop ileostomy is typically not required.
Radiographic features
The appearances described here are of the normal postoperative state.
Plain radiograph
Absence of normal gas pattern of the right colon. Surgical staples may be visible at the anastomosis site.
CT/MRI
The appendix, caecum and ascending colon will be absent, and other mobile abdominal structures may have moved to fill the resulting space 3. The anastomosis is generally found in the mid-abdomen but will depend on the extent to which the transverse colon was mobilised during the operation. The anastomosis may be more prominent if staples are used to divide and anastomose the bowel, but hand-sewn anastomoses will not be so visible. The ileocaecal valve will not be present so the reflux of colonic contents into the ileum will be possible.
Complications
anastomotic leak (~4% 2) - typically occurs in the first 2-3 weeks postoperatively 1
bleeding
wound infection


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}