
Sphenoid wing dysplasia is a characteristic but not pathognomonic feature of neurofibromatosis type 1 (NF1), it can also occur in isolated cases.
On this page:
Epidemiology
Sphenoid wing dysplasia is seen in 5-10% of cases of NF1 and is one of the diagnostic criteria of NF1 5,6.
Clinical presentation
Pulsatile exophthalmos is the most frequent presenting complaint 3. This occurs due to herniation of the temporal lobe into the orbit 5.
Pathology
Its exact aetiology is not clear. It can be seen isolated or associated with underlying plexiform neurofibroma.
Radiographic features
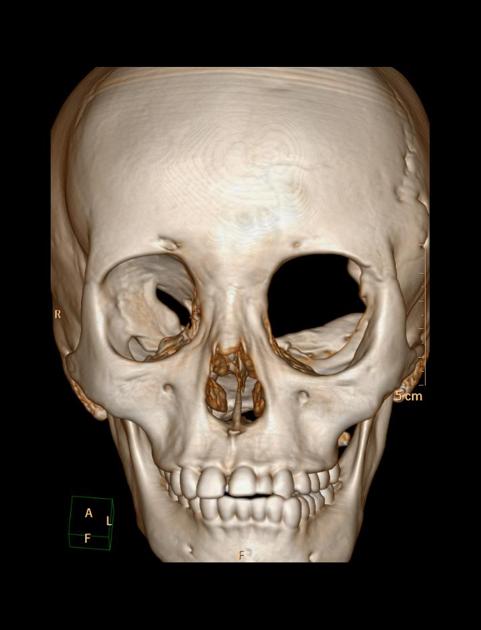
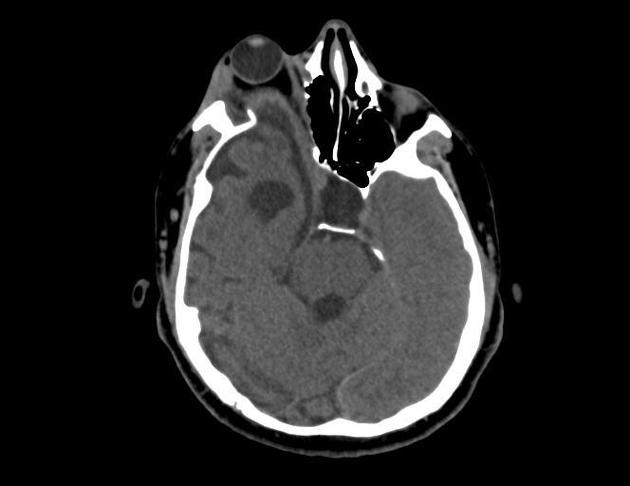
hypoplastic/absent sphenoid wing resulting in widening of the superior orbital fissure, elevation of the lesser sphenoid wing and ipsilateral orbital enlargement 3
gapping bony defect in the posterior aspect of the orbit 4
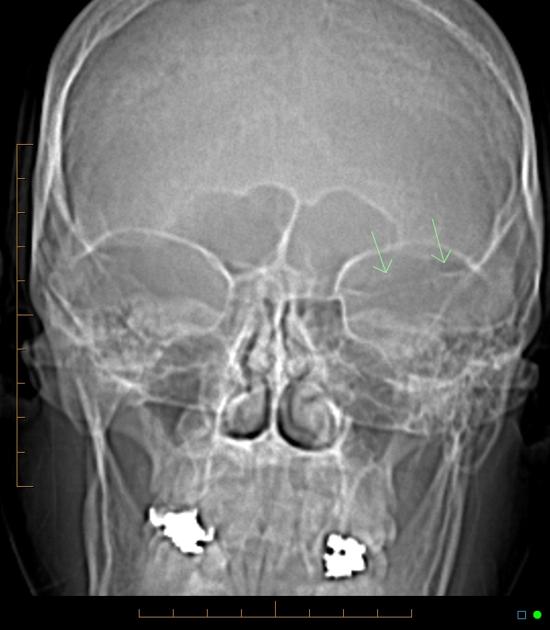
absence of the innominate line (which represents the projection of the greater wing of the sphenoid bone) on plain radiograph and CT scan giving the bare orbit sign 2
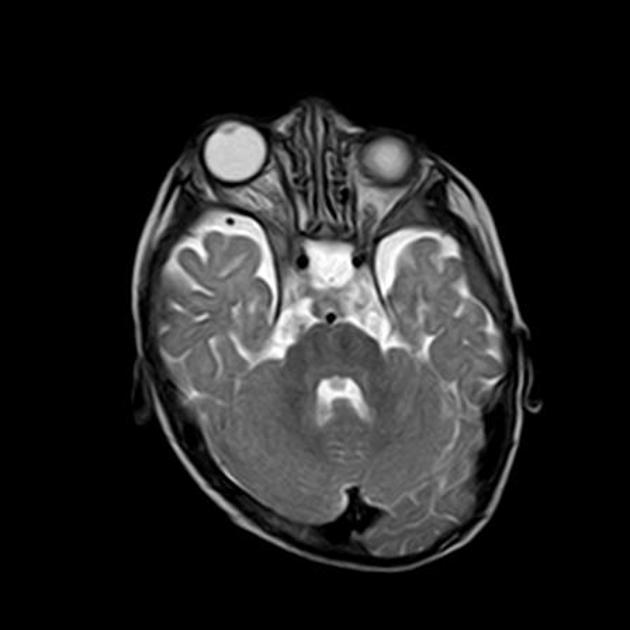
expansion and anteroposterior enlargement of the middle cranial fossa, usually associated with anterior temporal arachnoid cysts 1
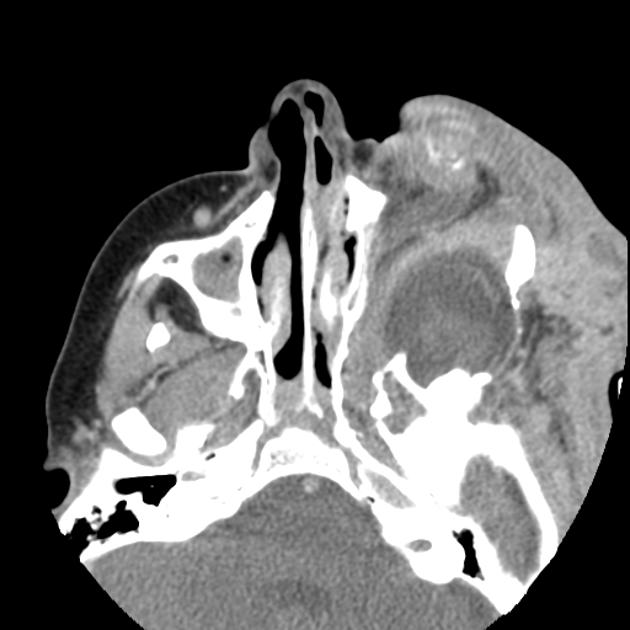
herniation of the dura, peritemporal subarachnoid space or the temporal lobe into the posterior aspect of the orbit, causing anterior displacement of the orbital contents 2
sphenoid wing dysplasia is usually associated with neurofibromas in the ipsilateral superficial temporal fossa which are often contiguous with a radiologically abnormal temporo-squamosal suture1





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.