
Thoracic endometriosis is an uncommon location for endometriosis and the main cause of catamenial pneumothorax.
On this page:
Epidemiology
Most often occurs in the third and fourth decades of life 3.
Clinical presentation
Symptoms may include:
- catamenial pleuritic chest pain
- catamenial haemoptysis: when endometrial tissue is in the bronchial tree
Patients may also present with a catamenial pneumothorax or catamenial haemothorax when endometrial tissue is in the lung periphery. The presentation may also be with a lung nodule.
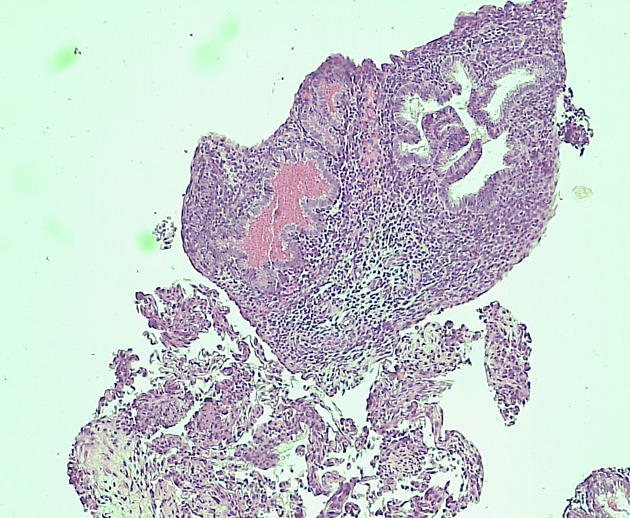
Pathology
Endometriosis is the presence of functioning endometrial tissue in extrauterine locations. It is most often confined to the pelvis; however extrapelvic sites like umbilicus, scar sites in abdomen, breasts, extremities and thorax may also be involved. In thorax the sites to be involved are pleura, parenchyma, airways and the diaphragm 1.
The exact pathogenesis of thoracic endometriosis is elusive. The theories postulated are:
- due to in utero pleural metaplasia into pleural endometrial tissue
- retrograde menstruation with further thoracic implantation of endometrial tissue by transdiaphragmatic passage
- hematogenic migration post a surgical gynaecological procedure
Post-implantation of endometrial tissue there is extensive decidual adhesions and distortion of tissue, which leads to the classical catamenial pain and haemoptysis 2.
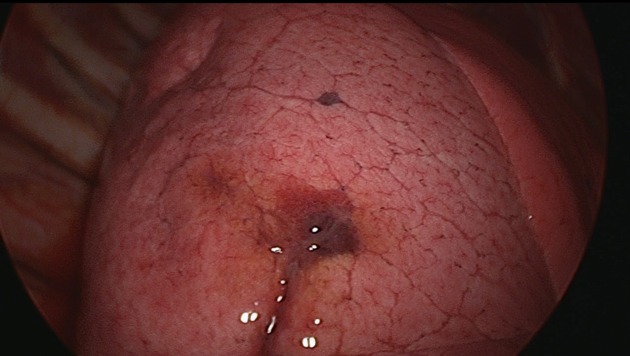
Location
There is a predilection for right-sided involvement in case of pleural endometriosis, however in parenchymal involvement there is no such predilection seen.
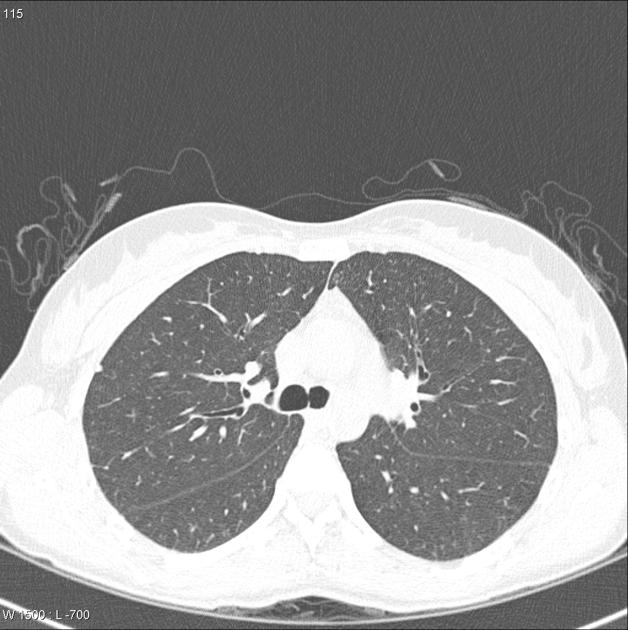
Radiographic features
CT
Chest CT is the modality of choice for thoracic endometriosis, which may demonstrate presence of pneumothorax, haemothorax or nodules which may change in nature cyclically. There may sometimes be vague areas of bronchial wall thickening, thin-walled cavities, bullous formation or ground glass opacities. CT may also be used to provide guidance for targeted biopsy. Imaging should be carried out during menstruation for higher sensitivity.
Treatment and prognosis
The treatment options are medical or surgical. Gonadotropin releasing hormone agonists are recommended for treatment of extrapelvic endometriosis. The other options are lung resection using VATS.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.