
The three-column concept of thoracolumbar spinal fractures (of Denis) forms the basis of several widely used thoracolumbar spinal fracture classification systems.
On this page:
Usage
While the three-column concept was initially developed for classifying thoracolumbar spinal fractures, it can also be applied to the lower cervical spine 3 as the general vertebral anatomy is similar to the thoracic and lumbar vertebrae. Due to its simplicity, it is widely used in routine clinical practice. It can be used in reports with the expectation that the treating clinicians will be familiar with the idea of anterior, middle and posterior columns.
The specific classification system Francis Denis described (see below) has been superseded by more modern classifications (AO classification of thoracolumbar injuries and the thoracolumbar injury classification and severity score). Yet, the three-column concept remains central to them.
Columns
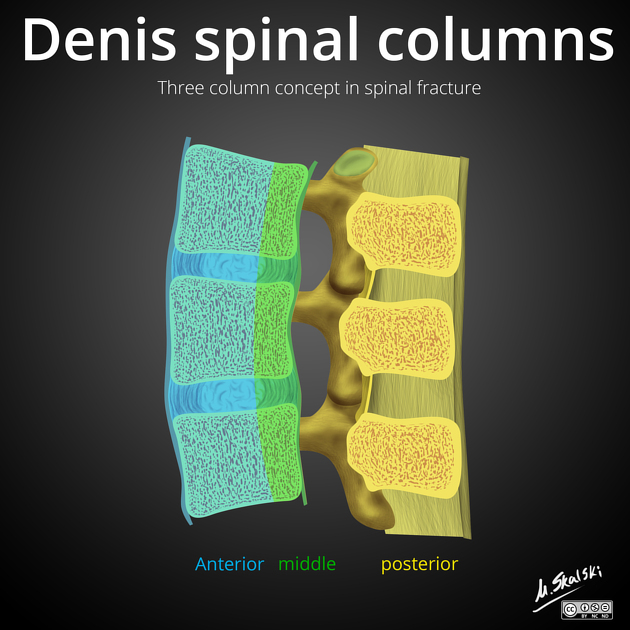
Denis divided the vertebral column into three vertical parallel columns based on biomechanical studies on stability following traumatic injury. Instability occurs when injuries affect two contiguous columns (e.g., the anterior and middle column or the middle and posterior column). Obviously, a three-column injury is also unstable.
The three columns are:
-
anterior column
anterior two-thirds of the vertebral body
anterior two-thirds of the intervertebral disc (annulus fibrosus)
-
middle column
posterior one-third of the vertebral body
posterior one-third of the intervertebral disc (annulus fibrosus)
-
posterior column
-
everything posterior to the PLL
pedicles
facet joints and articular processes
vertebral arch and interconnecting ligaments
-
Classification
Only of historical interest, it is worth noting that in the original 1976 article 1, Denis differentiated five types of fractures A-E:
-
type A
fracture of both endplates without kyphosis
mechanism of injury: pure axial load
predilection site: low lumbar region
-
type B
fracture of the superior endplate (CT may also demonstrate a sagittal split of the lower endplate)
most frequent burst fracture
mechanism of injury: axial load and flexion
predilection site: thoracolumbar junction
-
type C
fracture of the inferior endplate
rare
mechanism of injury: probably axial load and flexion.
no particular site pattern could be identified
-
type D
burst rotation fracture
burst fracture with comminution of the vertebral body, large central defect on CT, loss of posterior height, an increase of the interpedicular distance, vertical fracture of the lamina, bone retropulsed into the spinal canal
mechanism of injury: axial load and rotation
predilection site: mid lumbar region
-
type E
burst lateral flexion fracture
fractured posterior wall of the vertebral body with fragment extrusion towards the side of the flexion
mechanism of injury: axial load and lateral flexion




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.